

")



Случай спонтанного разрыва печени и роль визуализации: от компьютерной томографии до интервенционного лечения
- Авторы: Montatore M.1, Masino F.1, Muscatella G.1, Gifuni R.1, Tupputi R.2, Quinto F.3, Guglielmi G.1,2,4
-
Учреждения:
- Foggia University School of Medicine
- Dimiccoli Hospital
- L. Bonomo Hospital
- IRCCS Casa Sollievo della Sofferenza Hospital
- Выпуск: Том 5, № 3 (2024)
- Страницы: 632-641
- Раздел: Клинические случаи и серии клинических случаев
- URL: https://journals.rcsi.science/DD/article/view/310042
- DOI: https://doi.org/10.17816/DD623377
- ID: 310042
Цитировать
Полный текст

Аннотация
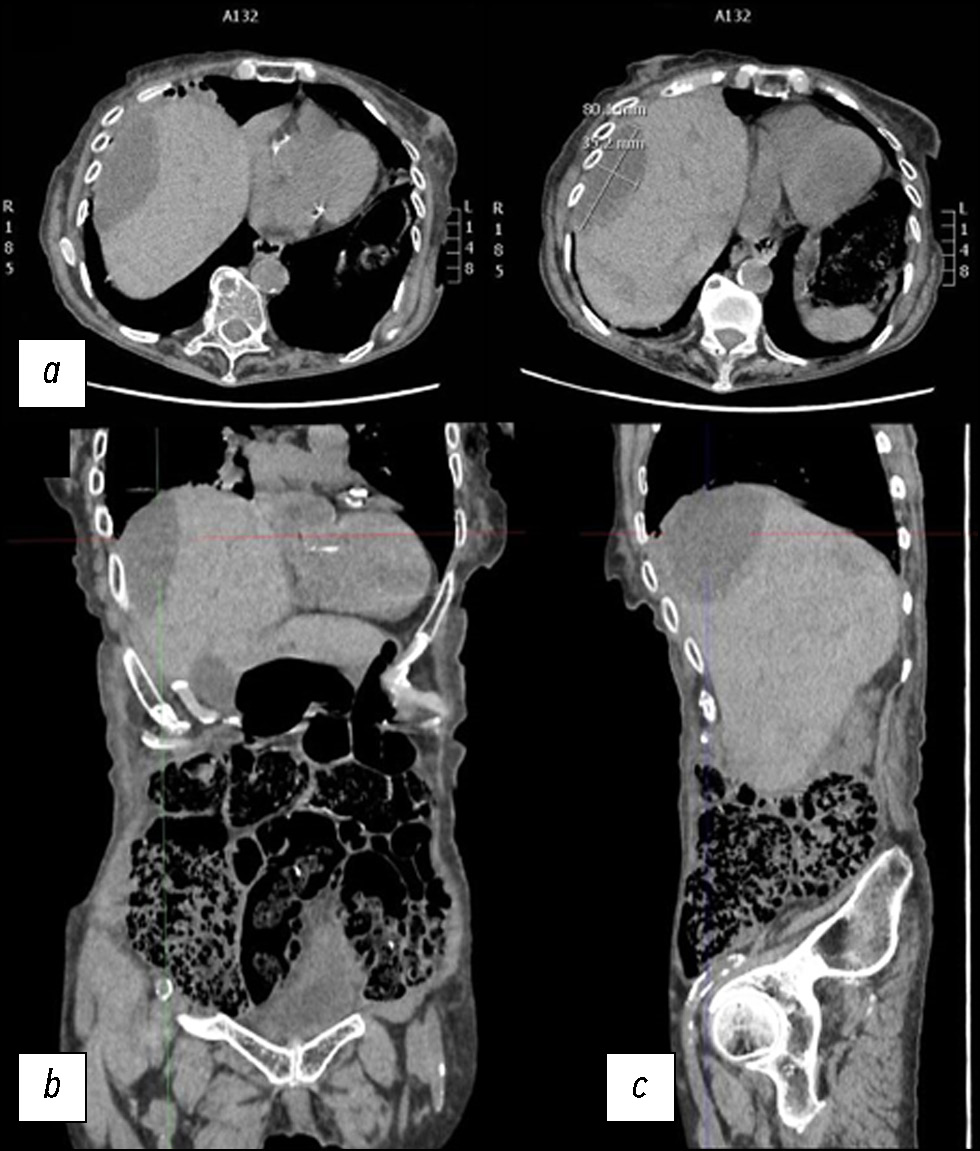
Разрыв паренхимы печени — редкое, но потенциально смертельное состояние, которое может быть вызвано травмой, ятрогенными факторами, спонтанными причинами и так далее. В данной статье описан клинический случай, в котором представлены диагностические и терапевтические меры, применённые в ходе лечения пациентки со спонтанным разрывом паренхимы печени. Пожилая женщина поступила в отделение неотложной помощи с болью в животе диффузного характера. После клинического обследования ей была проведена компьютерная томография. По результатам первой компьютерной томографии не выявили полномасштабного разрыва паренхимы. Из-за неоднозначности данных, указывающих на то, что боль в животе могла быть вызвана почечной или желчной коликой, поставить ранний диагноз было очень проблематично. В паренхиме печени было обнаружено лишь несколько гиподенсных образований овальной формы, наполненных жидкостью повышенной плотности. Однако боль сохранялась в течение нескольких дней, и ввиду ухудшения состояния пациентки были проведены дополнительные рентгенологические исследования, по результатам которых выявили разрыв паренхимы печени. Это потребовало в дальнейшем применения метода артериографии, а также длительного пребывания в стационаре до клинического разрешения.
Ключевые слова
Полный текст
Открыть статью на сайте журналаОб авторах
Manuela Montatore
Foggia University School of Medicine
Email: manuela.montatore@unifg.it
ORCID iD: 0009-0002-1526-5047
MD
Италия, ФоджаFederica Masino
Foggia University School of Medicine
Email: federicamasino@gmail.com
ORCID iD: 0009-0004-4289-3289
MD
Италия, ФоджаGianmichele Muscatella
Foggia University School of Medicine
Email: muscatella94@gmail.com
ORCID iD: 0009-0004-3535-5802
MD
Италия, ФоджаRossella Gifuni
Foggia University School of Medicine
Email: rossella.gifuni@unifg.it
ORCID iD: 0009-0009-9679-3861
MD
Италия, ФоджаRuggiero Tupputi
Dimiccoli Hospital
Email: rutudott@gmail.com
ORCID iD: 0009-0006-0329-6320
MD
Италия, БарлеттаFabio Quinto
L. Bonomo Hospital
Email: fabio.quinto@aslbat.it
ORCID iD: 0000-0001-7730-7711
MD
Италия, АндрияGiuseppe Guglielmi
Foggia University School of Medicine; Dimiccoli Hospital; IRCCS Casa Sollievo della Sofferenza Hospital
Автор, ответственный за переписку.
Email: giuseppe.guglielmi@unifg.it
ORCID iD: 0000-0002-4325-8330
профессор
Италия, Фоджа; Барлетта; Сан-Джованни-РотондоСписок литературы
- Fundora W., Fuster-Anglada C., Bassaganyas C., et al. An infrequent cause of spontaneous liver rupture // Journal of hepatology. 2023. Vol. 78, N 5. P. e160–e161. doi: 10.1016/j.jhep.2023.01.012
- Onishi Y., Shimizu H., Oka S., et al. Transcatheter arterial embolization for subcapsular hematoma of the liver // Abdominal radiology. 2023. Vol. 48, N 2. P. 765–772. doi: 10.1007/s00261-022-03732-w
- Le A.C.M., Bohlin T., Grønvold L., et al. Ruptured liver // Tidsskr Nor Laegeforen. 2023. Vol. 143, N 8. doi: 10.4045/tidsskr.22.0805
- Sutton B.C., Dunn S.T., Landrum J., Mielke G. Fatal postpartum spontaneous liver rupture: case report and literature review // Journal of forensic sciences. 2008. Vol. 53, N 2. P. 472–475. doi: 10.1111/j.1556-4029.2008.00677.x
- Donati M., Stavrou G.A., Donati A., Oldhafer K.J. The risk of spontaneous rupture of liver hemangiomas: a critical review of the literature // Journal of hepato-biliary-pancreatic sciences. 2011. Vol. 18, N 6. P. 797–805. doi: 10.1007/s00534-011-0420-7
- Jun C.H., Yoon J.H., Wi J.W., et al. Risk factors and clinical outcomes for spontaneous rupture of pyogenic liver abscess // Journal of digestive diseases. 2015. Vol. 16, N 1. P. 31–36. doi: 10.1111/1751-2980.12209
- Seifeddine B., Amel C., Ghofrane T., et al. Spontaneous rupture of hydatid cyst of liver in the peritoneal cavity with intact proligerous membrane: about a case and literature review // The Pan African medical journal. 2018. Vol. 30. P. 174. doi: 10.11604/pamj.2018.30.174.15054
- Cadili A., Gates J. The Role of Angioembolization in Hepatic Trauma // The American surgeon. 2021. Vol. 87, N 11. P. 1793–1801. doi: 10.1177/0003134820973729
- García I.C., Villalba J.S., Iovino D., et al. Liver Trauma: Until When We Have to Delay Surgery? A Review // Life (Basel). 2022. Vol. 12, N 5. P. 694. doi: 10.3390/life12050694
- Segalini E., Morello A., Leati G., et al. Primary angioembolization in liver trauma: major hepatic necrosis as a severe complication of a minimally invasive treatment narrative review // Updates in Surgery. 2022. Vol. 74, N 5. P. 1511–1519. doi: 10.1007/s13304-022-01372-9
- Parks R.W., Chrysos E., Diamond T. Management of liver trauma // The British journal of surgery. 1999. Vol. 86, N 9. P. 1121–1135. doi: 10.1046/j.1365-2168.1999.01210.x
Дополнительные файлы







