

")



Safety and efficacy of percutaneous vesselplasty (Vessel-X) in the treatment of symptomatic thoracolumbar vertebral fractures
- Authors: Masala S.1, Lacchè A.1, Zini C.1, Mannatrizio D.1, Marcia S.1, Bellini M.1, Guglielmi G.1
-
Affiliations:
- University of Foggia
- Issue: Vol 3, No 2 (2022)
- Pages: 98-107
- Section: Original Study Articles
- URL: https://journals.rcsi.science/DD/article/view/88685
- DOI: https://doi.org/10.17816/DD88685
- ID: 88685
Cite item

Abstract
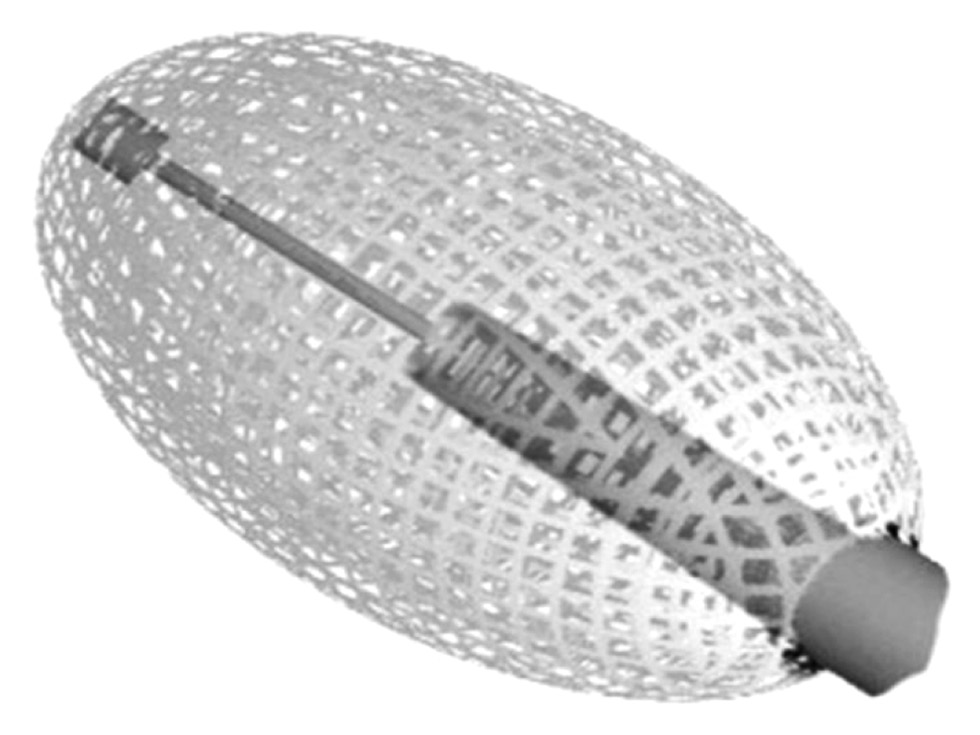
AIMS: to assess radiological and clinical outcomes, in terms of safety and efficacy, of symptomatic vertebral fractures with and without posterior wall and\or both endplates involvement, treated with vesselplasty technique (Vessel-X, Dragon Crown Medical Co., Ltd Shandong, China).
MATERIALS AND METHODS: We retrospectively evaluated 66 Patients who underwent 92 vesselplasty procedures, performed for the treatment of symptomatic vertebral body fractures from March 19 to September 2020. We divided the fractures in two subgroups: 36 vertebral fractures with posterior wall and/or both endplates involvement, which we defined complex, while all the others were defined simple. Numerical Rating Scale (NRS) and Oswestry Disability Index (ODI) values has been registered 1 day before the procedure and at 1, 6 and 12 months follow-up. We also evaluated vertebral height restoration by comparing pre-interventional with post-interventional imaging.
RESULTS: 92 vertebrae were treated (58 lumbar, 34 thoracic), with 24 multilevel procedures. We observed a technical success rate of 100%, without major complications; a single case of asymptomatic paravertebral cement leak was reported. Both simple and complex subgroups registered a significative statistical difference in NRS and ODI between preoperative and at 1, 6 and 12 months (p <0.05). A significant statistical difference was demonstrated in vertebral height comparing pre-operative and post-operative data (p <0.05). No significant difference in vertebral height restoration was observed between simple and complex vertebral fractures groups.
CONCLUSIONS: Vesselplasty represents a safe and effective technique for the treatment of both simple and complex painful vertebral fractures, granting a significant reduction of symptoms, excellent cement leakage control and proper vertebral height restoration.
Full Text
##article.viewOnOriginalSite##About the authors
Salvatore Masala
University of Foggia
Email: salva.masala@tiscali.it
ORCID iD: 0000-0003-0032-7970
MD
Italy, FoggiaAdriano Lacchè
University of Foggia
Email: adrianolacche@gmail.com
ORCID iD: 0000-0003-1782-8624
MD
Italy, FoggiaChiara Zini
University of Foggia
Email: zini.chiara@gmail.com
ORCID iD: 0000-0003-3456-4106
MD
Italy, FoggiaDomenico Mannatrizio
University of Foggia
Email: dr.mannatrizio@gmail.com
ORCID iD: 0000-0003-3365-7132
MD
Italy, FoggiaStefano Marcia
University of Foggia
Email: stemarcia@gmail.com
ORCID iD: 0000-0002-2118-9864
MD
Italy, FoggiaMatteo Bellini
University of Foggia
Email: matteo.bellini@icloud.com
ORCID iD: 0000-0002-1704-6246
MD
Italy, FoggiaGiuseppe Guglielmi
University of Foggia
Author for correspondence.
Email: giuseppe.guglielmi@unifg.it
ORCID iD: 0000-0002-4325-8330
MD, Professor
Italy, FoggiaReferences
- Kushchayev SV, Wiener PC, Teytelboym OM, et al. Percutaneous vertebroplasty: a history of procedure, technology, culture, specialty, and economics. Neuroimaging Clin N Am. 2019;29(4):481–494. doi: 10.1016/j.nic.2019.07.011
- Bornemann R, Koch EM, Wollny M, Pflugmacher R. Treatment options for vertebral fractures an overview of different philosophies and techniques for vertebral augmentation. Eur J Orthop Surg Traumatol. 2014;24(Suppl 1):S131–143. doi: 10.1007/s00590-013-1257-3
- Flors L, Lonjedo E, Leiva-Salinas C, et al. Vesselplasty: a new technical approach to treat symptomatic vertebral compression fractures. AJR Am J Roentgenol. 2009;193(1):218–226. doi: 10.2214/AJR.08.1503
- Tsoumakidou G, Too CW, Koch G, et al. CIRSE guidelines on percutaneous vertebral augmentation. Cardiovasc Intervent Radiol. 2017;40(3):331–342. doi: 10.1007/s00270-017-1574-8
- Filippiadis DK, Marcia S, Masala S, et al. Percutaneous vertebroplasty and kyphoplasty: current status, new developments and old controversies. Cardiovasc Intervent Radiol. 2017;40(12):1815–1823. doi: 10.1007/s00270-017-1779-x
- Diel P, Röder C, Perler G, et al. Radiographic and safety details of vertebral body stenting: results from a multicenter chart review. BMC Musculoskelet Disord. 2013;14:233. doi: 10.1186/1471-2474-14-233
- Vanni D, Galzio R, Kazakova A, et al. Third-generation percutaneous vertebral augmentation systems. J Spine Surg. 2016;2(1):13–20. doi: 10.21037/jss.2016.02.01
- Anselmetti GC, Manca A, Marcia S, et al. Vertebral augmentation with nitinol endoprosthesis: clinical experience in 40 patients with 1-year follow-up. Cardiovasc Intervent Radiol. 2014;37(1):193–202. doi: 10.1007/s00270-013-0623-1
- Zhan Y, Jiang J, Liao H, et al. Risk factors for cement leakage after vertebroplasty or kyphoplasty: a meta-analysis of published evidence. World Neurosurg. 2017;101:633–642. doi: 10.1016/j.wneu.2017.01.124
- Tempesta V, Cannata G, Ferraro G, et al. The new Vessel-X kyphoplasty for vertebral compression fractures: 2-year follow-up of 136 levels. Las Vegas: American Academy of Orthopaedic Surgeons Annual Meeting; 2009.
- McCall T, Cole C, Dailey A. Vertebroplasty and kyphoplasty: a comparative review of efficacy and adverse events. Curr Rev Musculoskelet Med. 2008;1:17–23. doi: 10.1007/s12178-007-9013-0
- Mroz TE, Yamashita T, Davros WJ, Lieberman IH. Radiation exposure to the surgeon and the patient during kyphoplasty. J Spinal Disord Tech. 2008;21(2):96–100. doi: 10.1097/BSD.0b013e31805fe9e1
- Ruiz Santiago F, Santiago Chinchilla A, Guzmán Álvarez L, et al. Comparative review of vertebroplasty and kyphoplasty. World J Radiol. 2014;6(6):329–343. doi: 10.4329/wjr.v6.i6.329
- Hiwatashi A, Yoshiura T, Yamashita K, et al. Morphologic change in vertebral body after percutaneous vertebroplasty: follow-up with MDCT. AJR Am J Roentgenol. 2010;195:W207–W212. doi: 10.2214/AJR.10.4195
- Grohs JG, Matzner M, Trieb K, Krepler P. Minimal invasive stabilization of osteoporotic vertebral fractures: a prospective nonrandomized comparison of vertebroplasty and balloon kyphoplasty. J Spinal Disord Tech. 2005;18(3):238–242.
- Lin EP, Ekholm S, Hiwatashi A, Westesson PL. Vertebroplasty: cement leakage into the disc increases the risk of new fracture of adjacent vertebral body. AJNR Am J Neuroradiol. 2004;25(2):175–180.
- Bambang D. Vesselplasty: a novel concept of percutaneous treatment for stabilization and height restoration of vertebral compression fractures. J Musculoskeletal Res. 2008;11(2):71–79. doi: 10.1142/s0218957708001985
- Zheng Z, Luk KD, Kuang G, et al. Vertebral augmentation with a novel Vessel-X bone void filling container system and bioactive bone cement. Spine (Phila Pa 1976). 2007;32(19):2076–2082. doi: 10.1097/BRS.0b013e3181453f64
- Carlier RY, Gordji H, Mompoint DM, et al. Osteoporotic vertebral collapse: percutaneous vertebroplasty and local kyphosis correction. Radiology. 2004;233(3):891–898. doi: 10.1148/radiol.2333030400
- Chen WJ, Kao YH, Yang SC, et al. Impact of cement leakage into disks on the development of adjacent vertebral compression fractures. J Spinal Disord Tech. 2010;23(1):35–39. doi: 10.1097/BSD.0b013e3181981843
- Komemushi A, Tanigawa N, Kariya S, et al. Percutaneous vertebroplasty for osteoporotic compression fracture: multivariate study of predictors of new vertebral body fracture. Cardiovasc Intervent Radiol. 2006;29(4):580–585. doi: 10.1007/s00270-005-0138-5
- Guarnieri G, Masala S, Muto M. Update of vertebral cementoplasty in porotic patients. Interv Neuroradiol. 2015;21(3):372–380. doi: 10.1177/1591019915582364
Supplementary files






