

")


Chronic esophageal fistula as a rare cause of secondary osteomyelitis of the thoracic spine
- Авторлар: Zarya V.A.1, Gavrilov P.V.1, Makogonova M.E.1, Kozak A.R.1, Vishnevskiy A.A.1
-
Мекемелер:
- Saint-Petersburg State Research Institute of Phthisiopulmonology
- Шығарылым: Том 4, № 3 (2023)
- Беттер: 403-410
- Бөлім: Case reports
- URL: https://journals.rcsi.science/DD/article/view/254078
- DOI: https://doi.org/10.17816/DD430128
- ID: 254078
Дәйексөз келтіру

Аннотация
Infectious diseases affecting the spine are inflammatory destructive diseases that involved the organ and its structural elements as a result of infection by hematogenic, lymphogenic, or contact pathways, including may be a complication of surgical intervention. In arriving at an accurate diagnosis, it is extremely important to evaluate the anamnesis, the clinical picture, as well as the data of laboratory studies and radiation diagnostics in the aggregate.
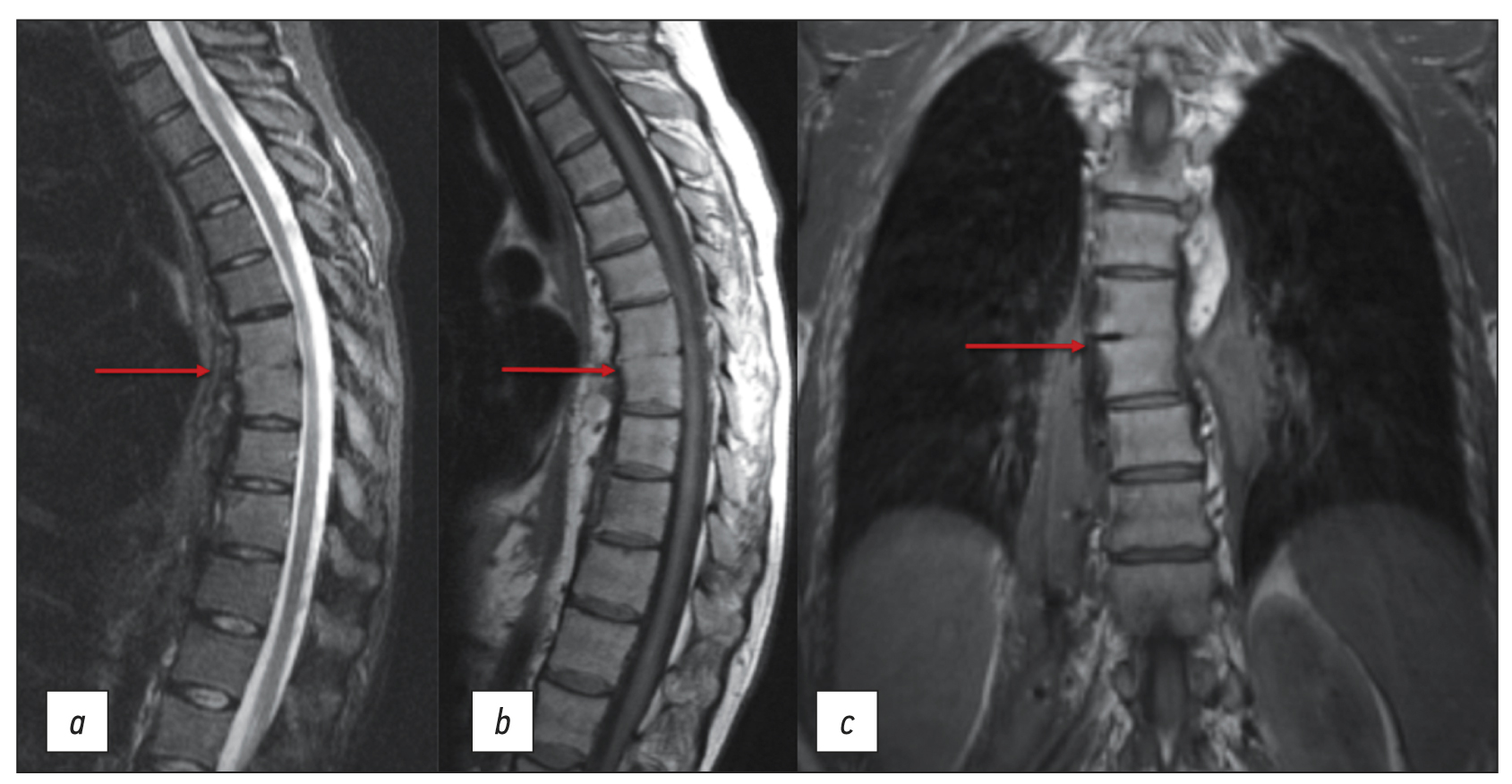
This article presents a clinical case with the development of secondary ThVII–ThVIII vertebral spondylitis due to esophageal fistula. At the initial diagnosis, spondylitis was associated with spinal anesthesia performed six months prior to onset of the disease, as there was a fistulous defect on the skin in the lumbar region. Consequently, surgical interventions were performed three times in a surgical hospital at the place of residence. The data from the endoscopic examination, as well as the patient’s complaints regarding the relationship between meals, the appearance of pain, and the nature of the discharge from the fistula were not taken into account by doctors initially. With the help of an additional examination, including computed tomography of the esophagus with oral contrast and computed tomography fistulography, the main diagnosis was esophageal fistula. Thoracic spondylitis was only a secondary complication.
Thus, the final diagnosis of back pain and fistula in the lumbar region should be formulated after differential diagnosis with alternative diseases of the spine.
Негізгі сөздер
Толық мәтін
##article.viewOnOriginalSite##Авторлар туралы
Valeriya Zarya
Saint-Petersburg State Research Institute of Phthisiopulmonology
Email: zariandra@mail.ru
ORCID iD: 0000-0001-7956-3719
Ресей, Saint Petersburg
Pavel Gavrilov
Saint-Petersburg State Research Institute of Phthisiopulmonology
Хат алмасуға жауапты Автор.
Email: spbniifrentgen@mail.ru
ORCID iD: 0000-0003-3251-4084
SPIN-код: 7824-5374
MD, Cand. Sci. (Med.)
Ресей, Saint PetersburgMarina Makogonova
Saint-Petersburg State Research Institute of Phthisiopulmonology
Email: MakogonovaME@gmail.com
ORCID iD: 0000-0001-6760-2426
SPIN-код: 6342-8967
MD, Cand. Sci. (Med.)
Ресей, Saint PetersburgAndrey Kozak
Saint-Petersburg State Research Institute of Phthisiopulmonology
Email: andrkozak@mail.ru
ORCID iD: 0000-0002-3192-1430
MD, Cand. Sci. (Med.)
Ресей, Saint PetersburgArkadiy Vishnevskiy
Saint-Petersburg State Research Institute of Phthisiopulmonology
Email: vichnevsky@mail.ru
ORCID iD: 0000-0002-9186-6461
SPIN-код: 4918-1046
MD, Dr. Sci. (Med.)
Ресей, Saint PetersburgӘдебиет тізімі
- Mushkin AYu, Vishnevsky AA. Clinical recommendations for the diagnosis of infectious spondylitis (draft for discussion). Medical Alliance. 2018;(3):65–74. (In Russ).
- Fowler VG, Justice A, Moore C, et al. Risk factors for hematogenous complications of intravascular catheter-associated Staphylococcus aureus bacteremia. Clin Infect Dis. 2005;40(5):695–703. doi: 10.1086/427806
- Lu YA, Hsu HH, Kao HK, et al. Infective spondylodiscitis in patients on maintenance hemodialysis: A case series. Ren Fail. 2017;39(1):179–186. doi: 10.1080/0886022X.2016.1256313
- Choi KB, Lee CD, Lee SH. Pyogenic spondylodiscitis after percutaneous endoscopic lumbar discectomy. J Korean Neurosurg Soc. 2010;48(5):455–460. doi: 10.3340/jkns.2010.48.5.455
- Hsieh MK, Chen LH, Niu CC, et al. Postoperative anterior spondylodiscitis after posterior pedicle screw instrumentation. Spine J. 2011;11(1):24–29. doi: 10.1016/j.spinee.2010.10.021
- Hanci M, Toprak M, Sarioğlu AC, et al. Oesophageal perforation subsequent to anterior cervical spine screw/plate fixation. Paraplegia. 1995;33(10):606–609. doi: 10.1038/sc.1995.128
- Orlando ER, Caroli E, Ferrante L. Management of the cervical esophagus and hypofarinx perforations complicating anterior cervical spine surgery. Spine. 2003;28:E290–E295. doi: 10.1097/00007632-200308010-00023
- Pompili A, Canitano S, Caroli F, et al. Asymptomatic esophageal perforation caused by late screw migration after anterior cervical plating: Report of a case and review of relevant literature. Spine. 2002;27:E499–E502. doi: 10.1097/00007632-200212010-00016
- Janssen I, Shiban E, Rienmüller A, et al. Treatment considerations for cervical and cervicothoracic spondylodiscitis associated with esophageal fistula due to cancer history or accidental injury: A 9-patient case series. Acta Neurochir (Wien). 2019;161(9):1877–1886. doi: 10.1007/s00701-019-03985-3
- Fonga-Djimi H, Leclerc F, Martinot A, et al. Spondylodiscitis and mediastinitis after esophageal perforation owing to a swallowed radiolucent foreign body. J Pediatr Surg. 1996;31(5):698–700. doi: 10.1016/s0022-3468(96)90677-6
- Wadie GM, Konefal SH, Dias MA, McLaughlin MR. Cervical spondylodiscitis from an ingested pin: A case report. J Pediatr Surg. 2005;40(3):593–596. doi: 10.1016/j.jpedsurg.2004.11.023
- Van Ooij A, Manni JJ, Beuls EA, Walenkamp GH. Cervical spondylodiscitis after removal of a fishbone. A case report. Spine (Phila Pa 1976). 1999;24(6):574–577. doi: 10.1097/00007632-199903150-00015
Қосымша файлдар





