

")



慢性食管瘘作为继发性胸椎骨髓炎的罕见病因
- 作者: Zarya V.A.1, Gavrilov P.V.1, Makogonova M.E.1, Kozak A.R.1, Vishnevskiy A.A.1
-
隶属关系:
- Saint-Petersburg State Research Institute of Phthisiopulmonology
- 期: 卷 4, 编号 3 (2023)
- 页面: 403-410
- 栏目: 临床病例及临床病例的系列
- URL: https://journals.rcsi.science/DD/article/view/254078
- DOI: https://doi.org/10.17816/DD430128
- ID: 254078
如何引用文章

详细
脊柱感染性疾病是由于血源性、淋巴原性或接触性感染(包括手术并发症)引起的器官及其结构元素的炎症性破坏性疾病。在进行诊断时,对病史、临床表现以及实验室检查和放射诊断数据进行评估极为重要。
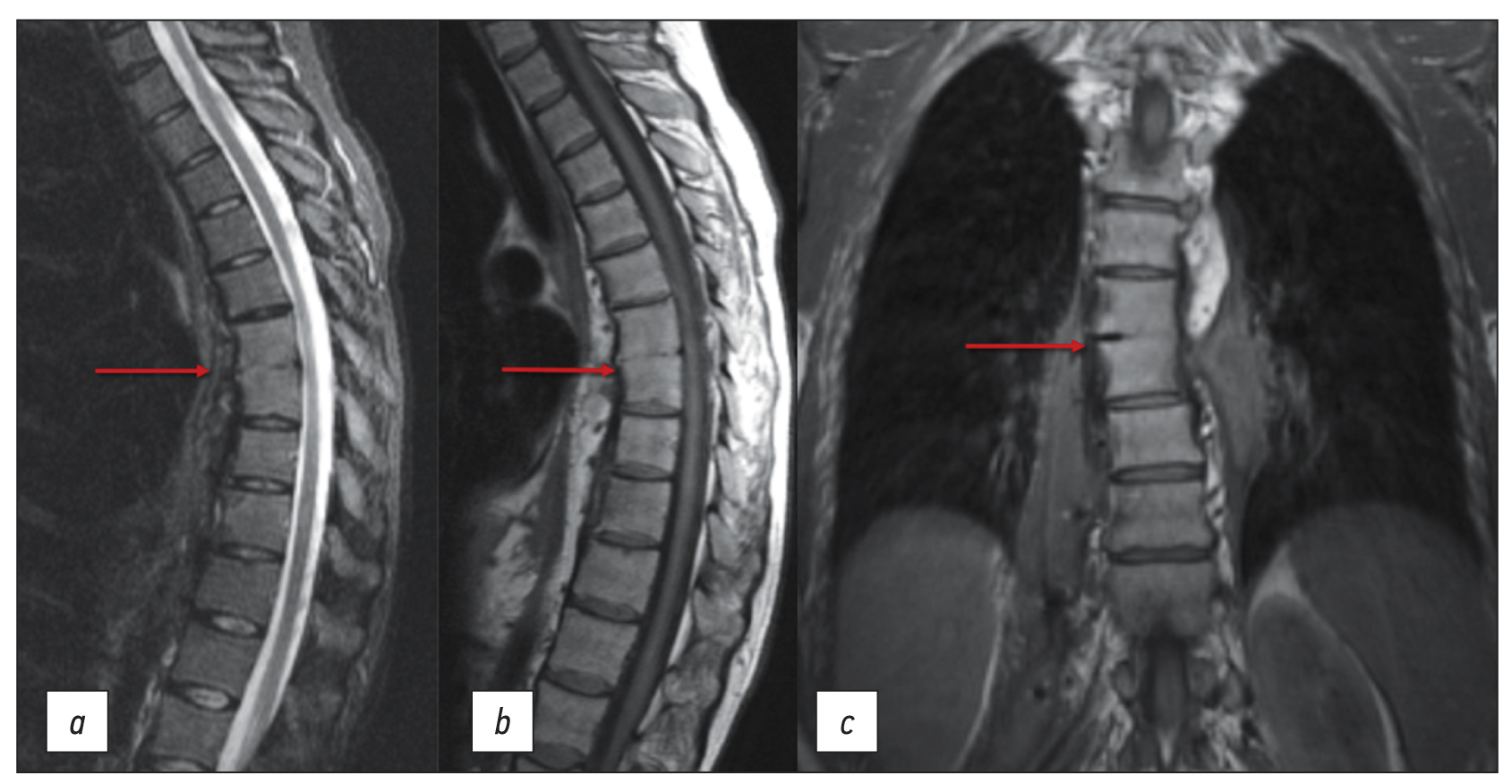
本文介绍一例因食管瘘引起的ThVII-ThVIII椎骨继发性脊椎炎的临床病例。在最初诊断时,医生认为脊椎炎与脊髓麻醉有关,而脊髓麻醉是在发病前6个月进行的,因为腰部皮肤上有瘘管缺损。这次在居住地的外科医院进行了三次手术治疗。医生最初并没有考虑到内窥镜检查结果以及病人关于进食、疼痛和瘘管分泌物性质之间关系的主诉。在额外检查的帮助下,包括口服造影剂的食道CT扫描和瘘管CT造影,确定了食管瘘的主要诊断,而胸椎脊椎炎只是次要并发症。
因此,在存在背痛的原因不仅是感染,还可能是手术治疗的并发症的情况下,最终诊断应该是在与其他脊柱疾病进行鉴别诊断后再做出的。
作者简介
Valeriya A. Zarya
Saint-Petersburg State Research Institute of Phthisiopulmonology
Email: zariandra@mail.ru
ORCID iD: 0000-0001-7956-3719
俄罗斯联邦, Saint Petersburg
Pavel V. Gavrilov
Saint-Petersburg State Research Institute of Phthisiopulmonology
编辑信件的主要联系方式.
Email: spbniifrentgen@mail.ru
ORCID iD: 0000-0003-3251-4084
SPIN 代码: 7824-5374
MD, Cand. Sci. (Med.)
俄罗斯联邦, Saint PetersburgMarina E. Makogonova
Saint-Petersburg State Research Institute of Phthisiopulmonology
Email: MakogonovaME@gmail.com
ORCID iD: 0000-0001-6760-2426
SPIN 代码: 6342-8967
MD, Cand. Sci. (Med.)
俄罗斯联邦, Saint PetersburgAndrey R. Kozak
Saint-Petersburg State Research Institute of Phthisiopulmonology
Email: andrkozak@mail.ru
ORCID iD: 0000-0002-3192-1430
MD, Cand. Sci. (Med.)
俄罗斯联邦, Saint PetersburgArkadiy A. Vishnevskiy
Saint-Petersburg State Research Institute of Phthisiopulmonology
Email: vichnevsky@mail.ru
ORCID iD: 0000-0002-9186-6461
SPIN 代码: 4918-1046
MD, Dr. Sci. (Med.)
俄罗斯联邦, Saint Petersburg参考
- Mushkin AYu, Vishnevsky AA. Clinical recommendations for the diagnosis of infectious spondylitis (draft for discussion). Medical Alliance. 2018;(3):65–74. (In Russ).
- Fowler VG, Justice A, Moore C, et al. Risk factors for hematogenous complications of intravascular catheter-associated Staphylococcus aureus bacteremia. Clin Infect Dis. 2005;40(5):695–703. doi: 10.1086/427806
- Lu YA, Hsu HH, Kao HK, et al. Infective spondylodiscitis in patients on maintenance hemodialysis: A case series. Ren Fail. 2017;39(1):179–186. doi: 10.1080/0886022X.2016.1256313
- Choi KB, Lee CD, Lee SH. Pyogenic spondylodiscitis after percutaneous endoscopic lumbar discectomy. J Korean Neurosurg Soc. 2010;48(5):455–460. doi: 10.3340/jkns.2010.48.5.455
- Hsieh MK, Chen LH, Niu CC, et al. Postoperative anterior spondylodiscitis after posterior pedicle screw instrumentation. Spine J. 2011;11(1):24–29. doi: 10.1016/j.spinee.2010.10.021
- Hanci M, Toprak M, Sarioğlu AC, et al. Oesophageal perforation subsequent to anterior cervical spine screw/plate fixation. Paraplegia. 1995;33(10):606–609. doi: 10.1038/sc.1995.128
- Orlando ER, Caroli E, Ferrante L. Management of the cervical esophagus and hypofarinx perforations complicating anterior cervical spine surgery. Spine. 2003;28:E290–E295. doi: 10.1097/00007632-200308010-00023
- Pompili A, Canitano S, Caroli F, et al. Asymptomatic esophageal perforation caused by late screw migration after anterior cervical plating: Report of a case and review of relevant literature. Spine. 2002;27:E499–E502. doi: 10.1097/00007632-200212010-00016
- Janssen I, Shiban E, Rienmüller A, et al. Treatment considerations for cervical and cervicothoracic spondylodiscitis associated with esophageal fistula due to cancer history or accidental injury: A 9-patient case series. Acta Neurochir (Wien). 2019;161(9):1877–1886. doi: 10.1007/s00701-019-03985-3
- Fonga-Djimi H, Leclerc F, Martinot A, et al. Spondylodiscitis and mediastinitis after esophageal perforation owing to a swallowed radiolucent foreign body. J Pediatr Surg. 1996;31(5):698–700. doi: 10.1016/s0022-3468(96)90677-6
- Wadie GM, Konefal SH, Dias MA, McLaughlin MR. Cervical spondylodiscitis from an ingested pin: A case report. J Pediatr Surg. 2005;40(3):593–596. doi: 10.1016/j.jpedsurg.2004.11.023
- Van Ooij A, Manni JJ, Beuls EA, Walenkamp GH. Cervical spondylodiscitis after removal of a fishbone. A case report. Spine (Phila Pa 1976). 1999;24(6):574–577. doi: 10.1097/00007632-199903150-00015
补充文件





