

")



Магнитно-резонансная томография при воронкообразной деформации грудной клетки
- Авторы: Музафарова Г.С.1, Вишнякова М.В.1, Абраменко А.С.1, Кузьмичев В.А.1, Гацуцын В.В.1
-
Учреждения:
- Московский областной научно-исследовательский клинический институт имени М.Ф. Владимирского
- Выпуск: Том 5, № 2 (2024)
- Страницы: 167-177
- Раздел: Оригинальные исследования
- URL: https://journals.rcsi.science/DD/article/view/264830
- DOI: https://doi.org/10.17816/DD568087
- ID: 264830
Цитировать

Аннотация
Обоснование. Магнитно-резонансная томография чаще применяется для подтверждения факта наличия воронкообразной деформации грудной клетки, а также для оценки компрессионных изменений сердца на этом уровне.
Цель — прицельная предоперационная оценка воронкообразной деформации грудной клетки по данным магнитно-резонансной томографии.
Материалы и методы. Проведена ретроспективная оценка магнитно-резонансной томографии органов грудной клетки у 38 пациентов (30 мужского пола, 8 женского пола). Средний возраст — 19,9 года (±9 лет).
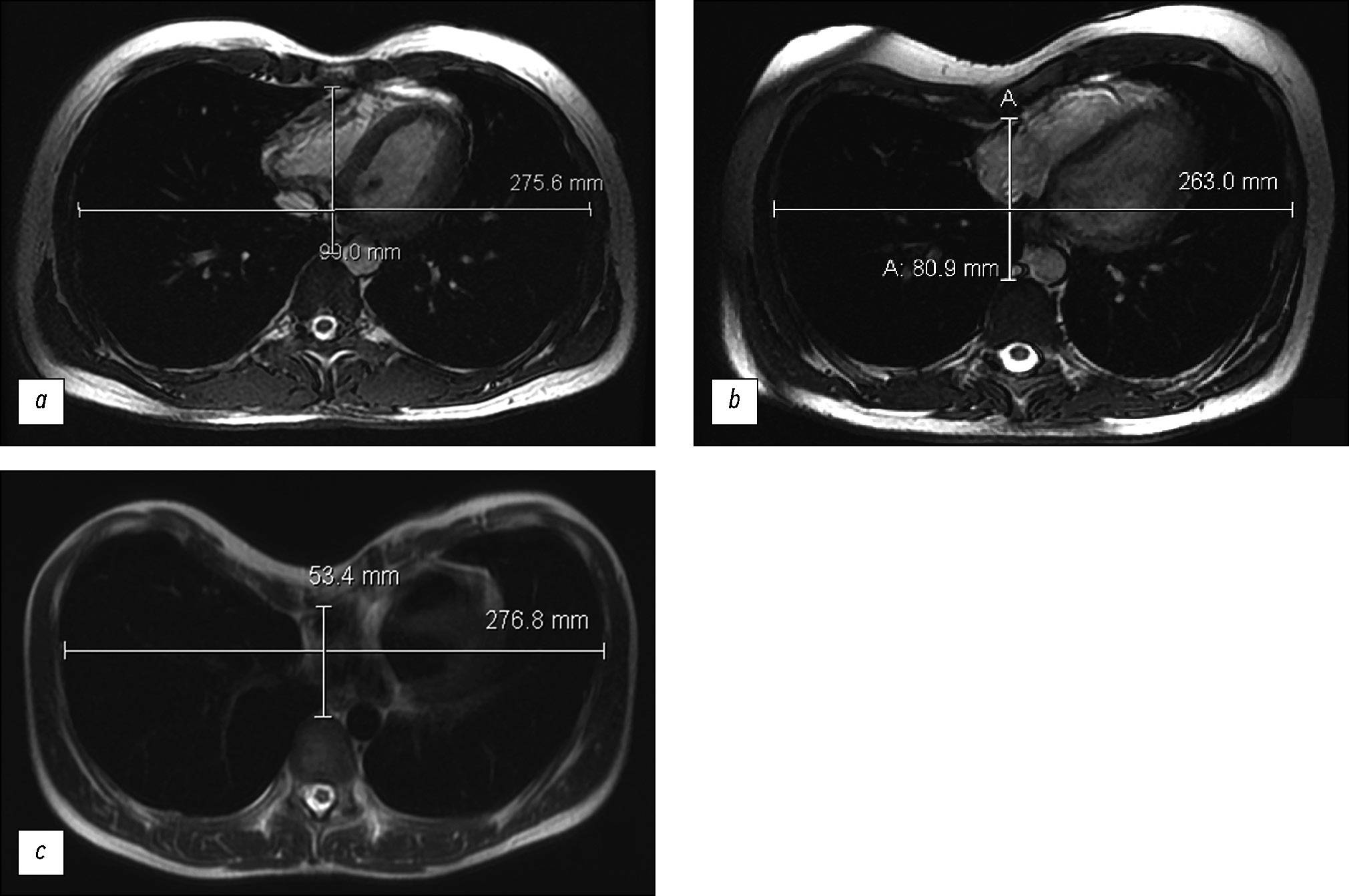
Магнитно-резонансная томография сердца выполнялась на аппарате General Electric Optima MR450w GEM 1,5 Тл с использованием импульсных последовательностей 2D-FIESTA-C с электрокардиографической синхронизацией с функциональной оценкой состояния левого и правого желудочков. Были получены параметры, необходимые для дальнейшего оперативного лечения пациентов по поводу воронкообразной деформации грудины — индекс Галлера, индекс коррекции, угол ротации грудины.
Проведена статистическая обработка полученных данных, поиск взаимосвязи между индексом Галлера, индексом коррекции, углом ротации грудины и фракцией выброса правого желудочка. Значение p <0,05 считали границей статистической значимости.
Результаты. В 92% случаев у пациентов выявлена умеренная и тяжёлая воронкообразная деформация грудной клетки. При поиске взаимосвязи между значениями индекса Галлера и фракцией выброса правого желудочка не было получено статистически значимой корреляции Пирсона (p=0,777 для значений фракции выброса на вдохе и p=0,798 для значений фракции выброса на выдохе). Среднее значение фракции выброса правого желудочка составило 46%.
При статистическом анализе по мере увеличения индекса Галлера (увеличение степени деформации органов грудной клетки) было отмечено увеличение индекса коррекции (p <0,05). Значения угла ротации грудины, потребовавшие модификации оперативного вмешательства (более 15°), были выявлены у 44,7% пациентов.
Заключение. Магнитно-резонансная томография — высокоинформативный метод диагностики при воронкообразной деформации грудной клетки: без лучевой нагрузки и с возможностью подробной предоперационной оценки патологических изменений.
Получены данные о наличии корреляции между значениями индекса Галлера и индекса коррекции (p <0,05). Кроме того, по данным магнитно-резонансной томографии выявлено уменьшение фракции выброса правого желудочка.
Полный текст
Открыть статью на сайте журналаОб авторах
Гулише Серверовна Музафарова
Московский областной научно-исследовательский клинический институт имени М.Ф. Владимирского
Email: gms0495@mail.ru
ORCID iD: 0000-0003-0940-3247
SPIN-код: 2950-5431
Россия, Москва
Марина Валентиновна Вишнякова
Московский областной научно-исследовательский клинический институт имени М.Ф. Владимирского
Автор, ответственный за переписку.
Email: cherridra@mail.ru
ORCID iD: 0000-0003-3838-636X
SPIN-код: 1137-2991
д-р мед. наук
Россия, МоскваАлександр Сергеевич Абраменко
Московский областной научно-исследовательский клинический институт имени М.Ф. Владимирского
Email: a.s.abramenko@gmail.com
ORCID iD: 0000-0002-6286-2162
SPIN-код: 9743-3001
Россия, Москва
Владимир Александрович Кузьмичев
Московский областной научно-исследовательский клинический институт имени М.Ф. Владимирского
Email: vakuzmichev@gmail.ru
ORCID iD: 0000-0001-6493-8012
SPIN-код: 8345-5298
канд. мед. наук, профессор
Россия, МоскваВладимир Витальевич Гацуцын
Московский областной научно-исследовательский клинический институт имени М.Ф. Владимирского
Email: vg86@list.ru
ORCID iD: 0000-0002-2364-5325
SPIN-код: 1431-4417
Россия, Москва
Список литературы
- Печетов А.А., Есаков Ю.С., Губайдуллина Г.Ф., Маков М.А., Хлань Т.Н. Выбор метода коррекции воронкообразной деформации грудной клетки у пациентов старшего возраста // Хирургия. Журнал им. Н.И. Пирогова. 2017. Т. 7. С. 24–29. doi: 10.17116/hirurgia2017724-29
- Fokin А.А., Steuerwald N.M., Ahrens W.A., Allen K.E. Anatomical, histologic, and genetic characteristics of congenital chest wall deformities // Seminars in Thoracic and Cardiovascular Surgery. 2009. Vol. 21, N 1. P. 44–57. doi: 10.1053/j.semtcvs.2009.03.001
- Scalise P.N., Demehri F.R. The management of pectus excavatum in pediatric patients: a narrative review // Transl Pediatr. 2023. Vol. 12, N 2. P. 208–220. doi: 10.21037/tp-22-361
- Trò R., Martini S., Stagnaro N., et al. A new tool for assessing Pectus Excavatum by a semi-automatic image processing pipeline calculating the classical severity indexes and a new marker: the Volumetric Correction Index // BMC Med Imaging. 2022. doi: 10.1186/s12880-022-00754-0
- Андреев П.С., Скворцов А.П., Цой И.В., и др. Лечение воронкообразной деформации грудной клетки у детей и подростков // Практическая медицина. 2021. Т. 19, № 4. С. 138–141. doi: 10.32000/2072-1757-2021-4-138-141
- Andreev P.S., Skvortsov A.Р., Khabibyanov R.Ya., Maleev M.V. Our experience in surgical treatment of penetral chest deformation // Annali d’Italia. 2023. N 41. P. 53–57. doi: 10.5281/zenodo.7774296
- Haller J.A. Jr, Kramer S.S., Lietman S.A., et al. Use of CT scans in selection of patients for pectus excavatum surgery: a preliminary report // J Pediatr Surg. 1987. Vol. 22, N 10. P. 904–906. doi: 10.1016/s0022-3468(87)80585-7
- Sidden C.R., Katz M.E., Swoveland B.C., Nuss D. Radiologic considerations in patients undergoing the Nuss procedure for correction of pectus excavatum // Pediatric Radiology. 2001. Vol. 31, N 6. P. 429–434. doi: 10.1007/s002470100455
- St. Peter S.D., Juang D., Garey C.L., et al. A novel measure for pectus excavatum: the correction index // Journal of Pediatric Surgery. 2011. Vol. 46, N 12. P. 2270–2273. doi: 10.1016/j.jpedsurg.2011.09.009
- Tauchi R., Suzuki Y., Tsuji T., et al. Clinical Characteristics and Thoracic factors in patients with Idiopathic and Syndromic Scoliosis Associated with Pectus Excavatum // Spine Surg Relat Res. 2018. Vol. 2, N 1. P. 37–41. doi: 10.22603/ssrr.2017-0027
- Шамсиев А.М., Шамсиев Ж.А., Тураев Ю.А., Муталибов А.И., Бургутов М.Ж. Роль функциональных исследований кардиореспираторной системы при воронкообразной деформации грудной клетки // Журнал Проблемы биологии и медицины. 2017. Т. 1, № 93. С. 9–14.
- Peng R., Mardakhaev E., Shmukler A., Levsky J.M., Haramati L.B. Meeting ACR Dose Guidelines for CT Lung Cancer Screening in an Overweight and Obese Population // Acad Radiol. 2021. Vol. 28, N 3. P. 381–386. doi: 10.1016/j.acra.2020.02.009
- Mortellaro V.E., Iqbal C.W., Fike F.B., et al. The predictive value of Haller index in patients undergoing pectus bar repair for pectus excavatum // J Surg Res. 2011. Vol. 170, N 1. P. 104–106. doi: 10.1016/j.jss.2011.02.014
- Karakılıç A., Karaçam V., Ersöz H., et al. Determination of severity of deformity with rib length to costal cartilage length ratio in thorax deformities // Turk Gogus Kalp Damar Cerrahisi Derg. 2018. Vol. 26, N 2. P. 279–285. doi: 10.5606/tgkdc.dergisi.2018.15009
- Poston P.M., Patel S.S., Rajput M., et al. The correction index: setting the standard for recommending operative repair of pectus excavatum // Ann Thorac Surg. 2014. Vol. 97, N 4. P. 1176–1180. doi: 10.1016/j.athoracsur.2013.12.050
- Marcovici P.A., LoSasso B.E., Kruk P., Dwek J.R. MRI for the evaluation of pectus excavatum // Pediatric Radiology. 2011. Vol. 41. P. 757–758. doi: 10.1007/s00247-011-2031-5
- Lollert A., Funk J., Tietze N., et al. Morphologic assessment of thoracic deformities for the preoperative evaluation of pectus excavatum by magnetic resonance imaging // European Radiology. 2015. Vol. 25. P. 785–791. doi: 10.1007/s00330-014-3450-0
- Dore M., Triana J.P., Bret M., et al. Advantages of Cardiac Magnetic Resonance Imaging for Severe Pectus Excavatum Assessment in Children // Eur J Pediatr Surg. 2018. Vol. 28, N 1. P. 34–38. doi: 10.1055/s-0037-1604427
- Saleh R.S., Finn J.P., Fenchel M., et al. Cardiovascular magnetic resonance in patients with pectus excavatum compared with normal controls // J Cardiovasc Magn Reson. 2010. Vol. 12, N 1. doi: 10.1186/1532-429X-12-73
- Stagnaro N., Trocchio G., Torre M., et al. Cardiovascular MRI assessment of pectus excavatum in pediatric patients and postoperative simulation using vacuum bell // J Pediatr Surg. 2021. Vol. 56, N 9. P. 1600–1605. doi: 10.1016/j.jpedsurg.2020.11.017
Дополнительные файлы







