

")



Computed tomography in the diagnosis of fever of unknown origin: A case report
- Authors: Shumskaya Y.F.1, Kostikova N.V.2, Akhmedzyanova D.A.1, Suleymanova M.M.2, Fominykh E.V.2, Mnatsakanyan M.G.2, Reshetnikov R.V.1
-
Affiliations:
- Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
- The First Sechenov Moscow State Medical University (Sechenov University)
- Issue: Vol 4, No 3 (2023)
- Pages: 393-402
- Section: Case reports
- URL: https://journals.rcsi.science/DD/article/view/254077
- DOI: https://doi.org/10.17816/DD472068
- ID: 254077
Cite item

Abstract
Fever of unknown origin can be a symptom of at least 200 diseases. Positron emission tomography-computed tomography, although highly informative, may not be readily available as an imaging tool. We present a clinical case of giant cell arteritis where computed tomography played a key role in arriving at a diagnosis.
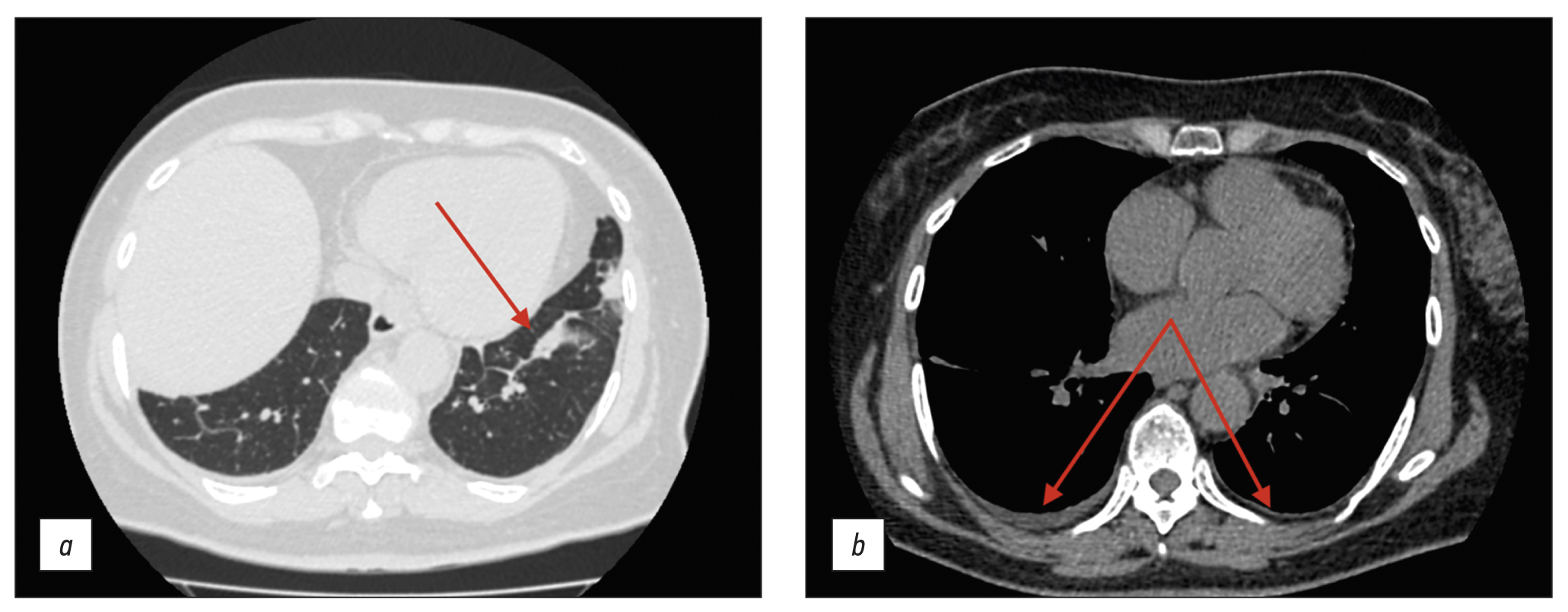
A 61-year-old woman presented to the hospital with a nocturnal fever up to 39.5°С, accompanied by chest and scapular pain, and substantial weight loss (10 kg over 3 months). Lymphoproliferative and infectious diseases were excluded. Baseline colonoscopy had revealed erosions in the colonic mucosa, leading to a preliminary diagnosis of ulcerative colitis, and subsequently, the patient was admitted to the gastroenterology department. Follow-up colonoscopy had excluded this diagnosis. Additional imaging via chest and abdominal computed tomography scan revealed wall thickening of aorta and its branches with subtle contrast enhancement.
Conditions, such as tuberculous aortoarteritis and syphilitic aortitis, were excluded. The patient was diagnosed with giant cell arteritis involving brachiocephalic trunk, subclavian arteries, and celiac trunk. Prednisolone was administered with subsequent reduction in symptoms.
Although computed tomography may not be regarded as the gold standard for the differential diagnosis of fever of unknown origin, this case underscores its valuable contribution in establishing a definitive diagnosis.
Full Text
##article.viewOnOriginalSite##About the authors
Yuliya F. Shumskaya
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
Author for correspondence.
Email: ShumskayaYF@zdrav.mos.ru
ORCID iD: 0000-0002-8521-4045
SPIN-code: 3164-5518
Russian Federation, Moscow
Nina V. Kostikova
The First Sechenov Moscow State Medical University (Sechenov University)
Email: n.kostikowa@yandex.ru
ORCID iD: 0000-0003-3509-7271
SPIN-code: 7962-4554
Russian Federation, Moscow
Dina A. Akhmedzyanova
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
Email: dina_akhm@mail.ru
ORCID iD: 0000-0001-7705-9754
SPIN-code: 6983-5991
Russian Federation, Moscow
Maria M. Suleymanova
The First Sechenov Moscow State Medical University (Sechenov University)
Email: ashe.danny.jush@gmail.com
ORCID iD: 0000-0002-5776-2693
SPIN-code: 7193-6122
Russian Federation, Moscow
Ekaterina V. Fominykh
The First Sechenov Moscow State Medical University (Sechenov University)
Email: evfominykh@mail.ru
ORCID iD: 0000-0003-3733-4381
Cand. Sci (Med.), Head of the Radiology Department
Russian Federation, MoscowMarina G. Mnatsakanyan
The First Sechenov Moscow State Medical University (Sechenov University)
Email: mnatsakanyan08@mail.ru
ORCID iD: 0000-0001-9337-7453
SPIN-code: 2015-1822
MD, Dr. Sci. (Med), Professor
Russian Federation, MoscowRoman V. Reshetnikov
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
Email: reshetnikov@fbb.msu.ru
ORCID iD: 0000-0002-9661-0254
SPIN-code: 8592-0558
Cand. Sci. (Phys.-Math.)
Russian Federation, MoscowReferences
- Unger M, Karanikas G, Kerschbaumer A, et al. Fever of unknown origin (Fuo) revised. Wien Klin Wochenschr. 2016;128(21-22):796–801. doi: 10.1007/s00508-016-1083-9
- David A, Quinlan JD. Fever of unknown origin in adults. Am Fam Physician. 2022;105(2):137–143.
- Fusco FM, Pisapia R, Nardiello S, et al. Fever of unknown origin (FUO): Which are the factors influencing the final diagnosis? A 2005–2015 systematic review. BMC Infect Dis. 2019;19(1):653. doi: 10.1186/s12879-019-4285-8
- Weitzer F, Hooshmand T, Pernthaler B, et al. Diagnostic value of F-18 FDG PET/CT in fever or inflammation of unknown origin in a large single-center retrospective study. Sci Rep. 2022;12(1):1883. doi: 10.1038/s41598-022-05911-7
- Wright WF, Auwaerter PG. Fever and fever of unknown origin: Review, recent advances, and lingering dogma. Open Forum Infect Dis. 2020;7(5):132. doi: 10.1093/ofid/ofaa132
- Horowitz HW. Fever of unknown origin or fever of too many origins? N Engl J Med. 2013;368(3):197–199. doi: 10.1056/NEJMp1212725
- Cunha BA, Lortholary O, Cunha CB. Fever of unknown origin: A clinical approach. Am J Med. 2015;128(10):1138.e1–1138.e15. doi: 10.1016/j.amjmed.2015.06.001
- Barber MS, Aronson JK, von Schoen-Angerer T, et al. CARE guidelines for case reports: explanation and elaboration document. Translation into Russian. Digital Diagnostics. 2022;3(1):16–42. (In Russ). doi: 10.17816/DD105291
- Shpilberg R, Hadjiyiannis D, Khan SA. Ulcerative colitis presenting as pyrexia of unknown origin (PUO) without bowel symptoms. Clin Med (Lond). 2012;12(4):389–390. doi: 10.7861/clinmedicine.12-4-389
- Soliman M, Shirazi-Nejad A, Bullas D, et al. An unusual case of pyrexia of unknown origin. Cureus. 2021;13(7):e16684. doi: 10.7759/cureus.16684
- Yavne Y, Tiosano S, Ben-Ami D, et al. Giant cell arteritis and inflammatory bowel disease: Is there a connection? Results from a population-based study. Autoimmun Rev. 2018;17(11):1134–1137. doi: 10.1016/j.autrev.2018.06.003
- Schäfer VS, Warrington KJ, Williamson EE, Kermani TA. Delayed diagnosis of biopsy-negative giant cell arteritis presenting as fever of unknown origin. J Gen Intern Med. 2009;24(4):532–536. doi: 10.1007/s11606-009-0925-9
- AlNuaimi D, Ansari H, Menon R, et al. Large vessel vasculitis and the rising role of FDG PET-CT: A case report and review of literature. Radiol Case Rep. 2020;15(11):2246–2249. doi: 10.1016/j.radcr.2020.08.066
- Grazioli-Gauthier L, Marcoli N, Vanini G, et al. Giant cell arteritis among fevers of unknown origin (FUO): An atypical presentation. Eur J Case Rep Intern Med. 2021;8(3):002254. doi: 10.12890/2021_002254
Supplementary files





