

")



电子计算机断层扫描在不明原因发热诊断中的应用:病例描述
- 作者: Shumskaya Y.F.1, Kostikova N.V.2, Akhmedzyanova D.A.1, Suleymanova M.M.2, Fominykh E.V.2, Mnatsakanyan M.G.2, Reshetnikov R.V.1
-
隶属关系:
- Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
- The First Sechenov Moscow State Medical University (Sechenov University)
- 期: 卷 4, 编号 3 (2023)
- 页面: 393-402
- 栏目: 临床病例及临床病例的系列
- URL: https://journals.rcsi.science/DD/article/view/254077
- DOI: https://doi.org/10.17816/DD472068
- ID: 254077
如何引用文章

详细
有两百多种疾病可以在不明原因发热的掩盖下发生。正电子发射断层扫描结合电子计算机断层扫描是诊断不明原因发热的一种信息丰富但并非总是可用的方法。本文介绍一例不明原因发热的女性患者,CT数据在她巨细胞动脉炎的诊断中发挥了关键作用。
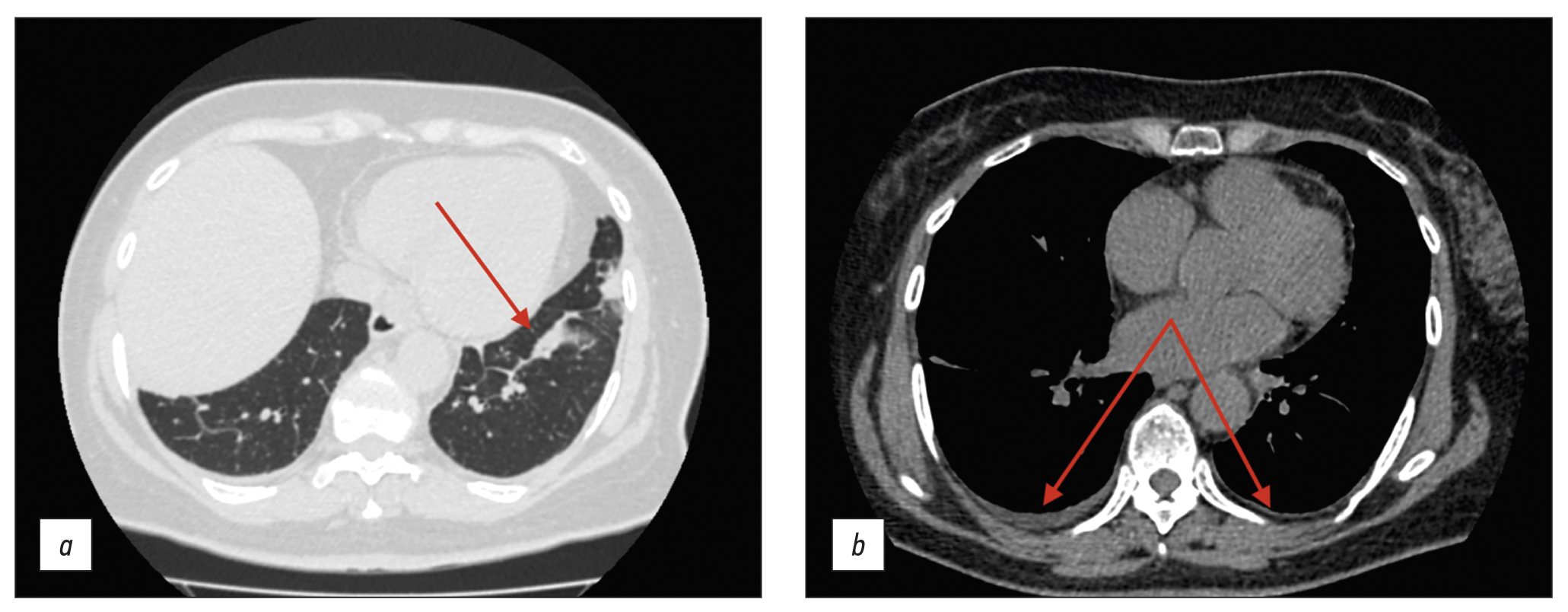
一名61岁的女性患者,主诉傍晚体温升高至39.5ºC,心前区和肩胛间区疼痛,体重在3个月内下降了10kg。在进行鉴别诊断时,排除了感染性疾病和淋巴增生性疾病。作为不明原因发热的原因,考虑了溃疡性结肠炎,该病曾在内窥镜检查中被发现,患者因此在消化科住院治疗。再次结肠镜检查显示了,内窥镜检查结果正常。通过静脉注射造影剂对胸腔和腹腔进行了电子计算机断层扫描,发现了主动脉及其分支的管壁明显增厚,造影剂积聚活跃,这反映了高度活跃的动脉炎。其他检查排除了特异性动脉炎。诊断结果为巨细胞动脉炎,并累及头臂干、锁骨下动脉和腹腔動脈干。医生给病人开了泼尼松龙,随后临床症状有所缓解。
虽然电子计算机断层扫描不是诊断不明原因发热的金标准,但在综合检查框架内使用这种方法,最终允许了对一名患有非典型巨细胞动脉炎病程和长期不明原因发热的患者确诊。
作者简介
Yuliya F. Shumskaya
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
编辑信件的主要联系方式.
Email: ShumskayaYF@zdrav.mos.ru
ORCID iD: 0000-0002-8521-4045
SPIN 代码: 3164-5518
俄罗斯联邦, Moscow
Nina V. Kostikova
The First Sechenov Moscow State Medical University (Sechenov University)
Email: n.kostikowa@yandex.ru
ORCID iD: 0000-0003-3509-7271
SPIN 代码: 7962-4554
俄罗斯联邦, Moscow
Dina A. Akhmedzyanova
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
Email: dina_akhm@mail.ru
ORCID iD: 0000-0001-7705-9754
SPIN 代码: 6983-5991
俄罗斯联邦, Moscow
Maria M. Suleymanova
The First Sechenov Moscow State Medical University (Sechenov University)
Email: ashe.danny.jush@gmail.com
ORCID iD: 0000-0002-5776-2693
SPIN 代码: 7193-6122
俄罗斯联邦, Moscow
Ekaterina V. Fominykh
The First Sechenov Moscow State Medical University (Sechenov University)
Email: evfominykh@mail.ru
ORCID iD: 0000-0003-3733-4381
Cand. Sci (Med.), Head of the Radiology Department
俄罗斯联邦, MoscowMarina G. Mnatsakanyan
The First Sechenov Moscow State Medical University (Sechenov University)
Email: mnatsakanyan08@mail.ru
ORCID iD: 0000-0001-9337-7453
SPIN 代码: 2015-1822
MD, Dr. Sci. (Med), Professor
俄罗斯联邦, MoscowRoman V. Reshetnikov
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
Email: reshetnikov@fbb.msu.ru
ORCID iD: 0000-0002-9661-0254
SPIN 代码: 8592-0558
Cand. Sci. (Phys.-Math.)
俄罗斯联邦, Moscow参考
- Unger M, Karanikas G, Kerschbaumer A, et al. Fever of unknown origin (Fuo) revised. Wien Klin Wochenschr. 2016;128(21-22):796–801. doi: 10.1007/s00508-016-1083-9
- David A, Quinlan JD. Fever of unknown origin in adults. Am Fam Physician. 2022;105(2):137–143.
- Fusco FM, Pisapia R, Nardiello S, et al. Fever of unknown origin (FUO): Which are the factors influencing the final diagnosis? A 2005–2015 systematic review. BMC Infect Dis. 2019;19(1):653. doi: 10.1186/s12879-019-4285-8
- Weitzer F, Hooshmand T, Pernthaler B, et al. Diagnostic value of F-18 FDG PET/CT in fever or inflammation of unknown origin in a large single-center retrospective study. Sci Rep. 2022;12(1):1883. doi: 10.1038/s41598-022-05911-7
- Wright WF, Auwaerter PG. Fever and fever of unknown origin: Review, recent advances, and lingering dogma. Open Forum Infect Dis. 2020;7(5):132. doi: 10.1093/ofid/ofaa132
- Horowitz HW. Fever of unknown origin or fever of too many origins? N Engl J Med. 2013;368(3):197–199. doi: 10.1056/NEJMp1212725
- Cunha BA, Lortholary O, Cunha CB. Fever of unknown origin: A clinical approach. Am J Med. 2015;128(10):1138.e1–1138.e15. doi: 10.1016/j.amjmed.2015.06.001
- Barber MS, Aronson JK, von Schoen-Angerer T, et al. CARE guidelines for case reports: explanation and elaboration document. Translation into Russian. Digital Diagnostics. 2022;3(1):16–42. (In Russ). doi: 10.17816/DD105291
- Shpilberg R, Hadjiyiannis D, Khan SA. Ulcerative colitis presenting as pyrexia of unknown origin (PUO) without bowel symptoms. Clin Med (Lond). 2012;12(4):389–390. doi: 10.7861/clinmedicine.12-4-389
- Soliman M, Shirazi-Nejad A, Bullas D, et al. An unusual case of pyrexia of unknown origin. Cureus. 2021;13(7):e16684. doi: 10.7759/cureus.16684
- Yavne Y, Tiosano S, Ben-Ami D, et al. Giant cell arteritis and inflammatory bowel disease: Is there a connection? Results from a population-based study. Autoimmun Rev. 2018;17(11):1134–1137. doi: 10.1016/j.autrev.2018.06.003
- Schäfer VS, Warrington KJ, Williamson EE, Kermani TA. Delayed diagnosis of biopsy-negative giant cell arteritis presenting as fever of unknown origin. J Gen Intern Med. 2009;24(4):532–536. doi: 10.1007/s11606-009-0925-9
- AlNuaimi D, Ansari H, Menon R, et al. Large vessel vasculitis and the rising role of FDG PET-CT: A case report and review of literature. Radiol Case Rep. 2020;15(11):2246–2249. doi: 10.1016/j.radcr.2020.08.066
- Grazioli-Gauthier L, Marcoli N, Vanini G, et al. Giant cell arteritis among fevers of unknown origin (FUO): An atypical presentation. Eur J Case Rep Intern Med. 2021;8(3):002254. doi: 10.12890/2021_002254
补充文件





