

")



磁共振成像诊断宫颈内膜腺癌的可能性和局限性
- 作者: Antonova I.B.1, Aksenova S.P.1, Nudnov N.V.1,2,3, Kriger A.V.1
-
隶属关系:
- Russian Scientific Center of Roentgenoradiology
- Peoples’ Friendship University of Russia
- Russian Medical Academy of Continuous Professional Education
- 期: 卷 5, 编号 2 (2024)
- 页面: 149-166
- 栏目: 原创性科研成果
- URL: https://journals.rcsi.science/DD/article/view/264829
- DOI: https://doi.org/10.17816/DD585195
- ID: 264829
如何引用文章

详细
论证。近几十年来,宫颈腺癌的发病率从 5% 上升到 20%。已证实宫颈内膜腺癌的特点是病程较长,转移较早。由于宫颈腺癌细胞学诊断的困难,放射诊断在诊断和分期阶段发挥着关键作用。迄今为止,关于磁共振成像在宫颈腺癌诊断中的应用的研究还很少。
目的是确定磁共振成像在根据 T 标准对宫颈腺癌进行分期时的诊断信息量,以及在评估肿瘤侵入宫颈基质的深度时的诊断信息量,明确腺癌的符号标志和肿瘤在子宫内生长的特殊性。
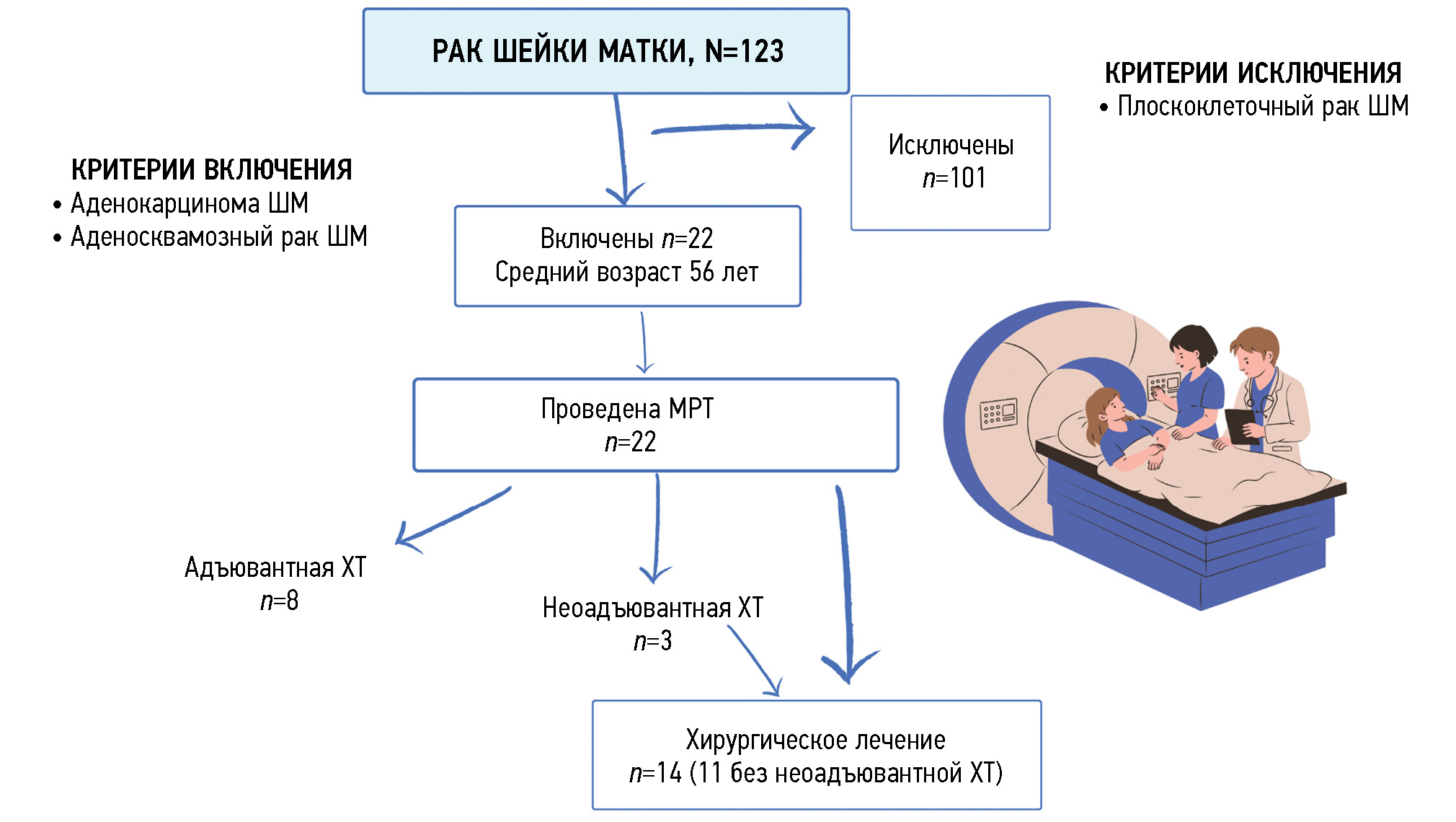
材料和方法。2020 年至 2023 年间,123 名确诊为宫颈癌(C53)的患者接受了检查。我们详细分析了 22 名(18%)宫颈腺癌患者(平均年龄 56 岁)使用 1.5 特斯拉磁场强度断层扫描仪接受盆腔器官磁共振成像的结果。对 11/22 例(50%)患者的磁共振成像信息分析进行了评估,这些患者接受了第一阶段手术治疗,切除了子宫和附件。为了分析诊断的信息量,对磁共振成像数据和手术材料的病理形态学检查数据进行了比较。研究结果的统计处理使用 Microsoft Excel 和 JavaStat 软件应用程序进行。
结果。磁共振成像在评估宫颈内膜腺癌局部患病率方面的信息量(根据 T 标准)为(以下主要值后的括号中给出了 95% 的置信区间):灵敏度为 77.78%(39.99%-97.19%);特异性为 50.00%(1.26%-98.74%);阳性结果预测值为 87.50%(62.64%-96.69%);阴性结果预测值为 33.33%(7.30%-76.04%);准确度为 72.73%(39.03%-93.98%)。磁共振成像在评估肿瘤侵入宫颈基质深度方面的信息量为:机会比率为 3.500(0.145-84.694);灵敏度为 85.7%(0.757-0.993),特异性为 33.3%(0.018-0.0648),阳性结果预测值为 75%(0.673-0.883),阴性结果预测值为 50%(0.027-0.972)。
结论。本研究表明了,磁共振成像是检测宫颈内膜腺癌的良好工具,具有很高的诊断信息量。在磁共振成像数据分析过程中发现的宫颈腺癌肿瘤生长宏观结构的 4 种类型表明,肿瘤生长具有局部侵袭性,向子宫内膜脱落的频率较高。这样就能为放射科医生提供描述性的图片结构,在宫颈腺癌得到证实的情况下也是如此,从而为患者制定更好的治疗方案。
作者简介
Irina B. Antonova
Russian Scientific Center of Roentgenoradiology
Email: Iran24@yandex.ru
ORCID iD: 0000-0003-2668-2110
SPIN 代码: 6247-3917
MD, Dr. Sci. (Medicine)
俄罗斯联邦, MoscowSvetlana P. Aksenova
Russian Scientific Center of Roentgenoradiology
编辑信件的主要联系方式.
Email: fabella@mail.ru
ORCID iD: 0000-0003-2552-5754
SPIN 代码: 4858-4627
MD, Cand. Sci. (Medicine)
俄罗斯联邦, MoscowNikolay V. Nudnov
Russian Scientific Center of Roentgenoradiology; Peoples’ Friendship University of Russia; Russian Medical Academy of Continuous Professional Education
Email: nvnudnov@rncrr.ru
ORCID iD: 0000-0001-5994-0468
SPIN 代码: 3018-2527
MD, Dr. Sci. (Medicine), Professor
俄罗斯联邦, Moscow; Moscow; MoscowAnna V. Kriger
Russian Scientific Center of Roentgenoradiology
Email: dr.akriger@gmail.com
ORCID iD: 0000-0001-6823-2658
SPIN 代码: 2338-6164
俄罗斯联邦, Moscow
参考
- Global health estimates: Leading causes of death. Cause-specific mortality, 2000–2019. World Health Organization; c2024. Available from: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-of-death
- Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi: 10.3322/caac.21660
- Kaprin AD, Starinskii VV, Shakhzadova AO, editors. State of oncological care for the Russian population in 2021. Moscow: MNIOI im. P.A. Gertsena — filial FGBU “NMITs radiologii” Minzdrava Rossii; 2022. (In Russ).
- Chan ZF, Zhi KZ. Prevalence and attribution of high-risk HPV in different histological types of cervical cancer. Zhonghua Fu Chan Ke Za Zhi. 2019;54(5):293–300. doi: 10.3760/cma.j.issn.0529-567x.2019.05.002
- Li N, Franceschi S, Howell-Jones R, et al. Human papillomavirus type distribution in 30,848 invasive cervical cancers worldwide: Variation by geographical region, histological type and year of publication. Int J Cancer. 2011;128(4):927–935. doi: 10.1002/ijc.25396
- Nicolás I, Marimon L, Barnadas E, et al. HPV-negative tumors of the uterine cervix. Mod Pathol. 2019;32(8):1189–1196. doi: 10.1038/s41379-019-0249-1
- NCCN guidelines panel. Cervical Cancer. Version 1.2021 PA: National Comprehensive Cancer Network; c2024. Available from: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1426
- Cervical cancer. Clinical guidelines. ID 537. Approved by the Scientific and Practical Council of the Ministry of Health of the Russian Federation. 2020. Available from: https://cr.minzdrav.gov.ru/recomend/537_1 (In Russ).
- Stolnicu S, Barsan I, Hoang L, et al. International Endocervical Adenocarcinoma Criteria and Classification (IECC): A New Pathogenetic Classification for Invasive Adenocarcinomas of the Endocervix. Am J Surg Pathol. 2018;42(2):214–226. doi: 10.1097/PAS.0000000000000986
- Grigoruk OG, Moskvina TA, Tsoy DA, et al. Endocervical adenocarcinomas. Cytological, histological, and molecular diagnostics. Tumors of female reproductive system. 2022;18(2):109–118. doi: 10.17650/1994-4098-2022-18-2-109-118
- World Health Organization. Female Genital Tumors. In: WHO Classification of Tumours, 5th Edition, Volume 4. International Agency for Research on Cancer; 2020.
- Islami F, Fedewa SA, Jemal A. Trends in cervical cancer incidence rates byage, race/ethnicity, histological subtype, and stage at diagnosis in the United States. Preventive Medicine. 2019;123:316–323. doi: 10.1016/j.ypmed.2019.04.010
- Hu J, Zheng P, Zhu L. Comparison of clinical pathological characteristics in ovarian preserving patients with stage IB1 cervical adenocarcinoma and squamous cell carcinoma. Journal of Peking University (Health Sciences). 2016;48(5):783–787. doi: 10.3969/j.issn.1671-167X.2016.05.006
- Hu K, Wang W, Liu X, et al. Comparison of treatment outcomes between squamous cell carcinoma and adenocarcinoma of cervix after definitive radiotherapy or concurrent chemoradiotherapy. Radiat Oncol. 2018;13(1):249. doi: 10.1186/s13014-018-1197-5
- Fan Y, Wang M, Mu Y, et al. Ovarian metastasis in women with cervical carcinoma in stages IA to IIB. Medicine (Baltimore). 2020;99(31):e21146. doi: 10.1097/MD.0000000000021146
- Bhatla N, Aoki D, Sharma DN, et al. Cancer of the cervix uteri: 2021 update. Int J Gynaecol Obstet. 2021;155 Suppl. 1:28–44. doi: 10.1002/ijgo.13865
- Stewart CJR, Crum CP, McCluggage WG, et al. Guidelines to Aid in the Distinction of Endometrial and Endocervical Carcinomas, and the Distinction of Independent Primary Carcinomas of the Endometrium and Adnexa From Metastatic Spread Between These and Other Sites. Int J Gynecol Pathol. 2019;38 Suppl. 1(1 Suppl. 1):S75–S92. doi: 10.1097/PGP.0000000000000553
- Song J, Im S, Lee SH, Jang HJ. Deep Learning-Based Classification of Uterine Cervical and Endometrial Cancer Subtypes from Whole-Slide Histopathology Images. Diagnostics (Basel). 2022;12(11):2623. doi: 10.3390/diagnostics12112623
- Woo S, Atun R, Ward ZJ, et al. Diagnostic performance of conventional and advanced imaging modalities for assessing newly diagnosed cervical cancer: systematic review and meta-analysis. Eur Radiol. 2020;30(10):5560–5577. doi: 10.1007/s00330-020-06909-3
- Merz J, Bossart M, Bamberg F, et al. Revised FIGO Staging for Cervical Cancer — A New Role for MRI. Rofo. 2020;192(10):937–944. doi: 10.1055/a-1198-5729
- Rubtsova NA, Novikova EG, Sinitsyn VE. MRI opportunities in cervical cancer local staging preoperative evaluation. Obstetrics, Gynecology and Reproduction. 2012;6(3):6–13. EDN: PUVJZT
- Balcacer P, Shergill A, Litkouhi B. MRI of cervical cancer with a surgical perspective: staging, prognostic implications and pitfalls. Abdom Radiol (NY). 2019;44(7):2557–2571. doi: 10.1007/s00261-019-01984-7
- Woo S, Suh CH, Kim SY, et al. Magnetic resonance imaging for detection of parametrial invasion in cervical cancer: An updated systematic review and meta-analysis of the literature between 2012 and 2016. European Radiology. 2018;28(2):530–541. doi: 10.1007/s00330-017-4958-x
- Alt CD, Bharwani N, Danza FM, et al. ESUR Quick Guide to Female Pelvis Imaging. ESUR, 2019. Available from: https://www.researchgate.net/publication/334725882_ESUR_Quick_Guide_to_Female_Pelvis_Imaging
- Castanon A, Landy R, Sasieni PD. Is cervical screening preventing adenocarcinoma and adenosquamous carcinoma of the cervix. Int J Cancer. 2016;139(5):1040–1045 doi: 10.1002/ijc.30152
- Suh DH, Ha HI, Lee YJ, et al. Incidence and treatment outcomes of uterine cervical cancer in Korea 1999–2018 from the national cancer registry. J Gynecol Oncol. 2023;34(2):e39. doi: 10.3802/jgo.2023.34.e39
- Miyamoto T, Kobara H, Shiozawa T. Biology and management of lobular endocervical glandular hyperplasia. J Obstet Gynaecol Res. 2022;48(12):3056–3067. doi: 10.1111/jog.15441
- Kerwin CM, Markese M, Moroney MR, et al. Adenocarcinoma of the uterine cervix, gastric-type (GAS): a review of the literature focused on pathology and multimodality imaging. Abdom Radiol (NY). 2023;48(2):713–723. doi: 10.1007/s00261-022-03724-w
- Marnitz S, Tsunoda AT, Martus P, et al. Surgical versus clinical staging prior to primary chemoradiation in patients with cervical cancer FIGO stages IIB–IVA: oncologic results of a prospective randomized international multicenter (Uterus-11) intergroup study. Int J Gynecol Cancer. 2020;30(12):1855–1861. doi: 10.1136/ijgc-2020-001973
- Akhavan S, Mousavi A, Sheikh Hassani S, et al. Evaluation of Cervical Cancer Staging Based on Magnetic Resonance Imaging in Comparison with Surgical Staging. Int J Cancer Manag. 2023;16(1):e126966. doi: 10.5812/ijcm-126966
- Trukhacheva NG, Frolova IG, Kolomiets LA, et al. Assessment of the extent of cervical cancer spread using magnetic resonance imaging. Siberian journal of oncology. 2015;(2):64–70. EDN: TSLSAD
- Horn LC, Höhn AK, Stark S, et al. Endocervical adenocarcinoma in situ (AIS) with ovarian and pulmonary involvement: report of a case and review of the literature suggesting a “seed and soil hypothesis”. J Cancer Res Clin Oncol. 2019;145(8):2061–2069. doi: 10.1007/s00432-019-02966-4
- Mao L, Zhang X, Chen T, et al. High-resolution reduced field-of-view diffusion-weighted magnetic resonance imaging in the diagnosis of cervical cancer. Quant Imaging Med Surg. 2023;13(6):3464–3476. doi: 10.21037/qims-22-579
- Kuang F, Ren J, Zhong Q, et al. The value of apparent diffusion coefficient in the assessment of cervical cancer. Eur Radiol. 2013;23(4):1050–1058. doi: 10.1007/s00330-012-2681-1
- Wang M, Perucho JAU, Chan Q. Diffusion Kurtosis Imaging in the Assessment of Cervical Carcinoma. Acad Radiol. 2020;27(5):E94–E101. doi: 10.1016/j.acra.2019.06.022
- Monist M, Lewkowicz D, Piętak P, et al. Synchronously occurring endometrioid carcinomas of the uterine corpus and uterine cervix preceded by different precancerous lesions: A case study and a literature review. Pathol Res Pract. 2023;245:154452. doi: 10.1016/j.prp.2023.154452
- Lin YC, Lin G, Chen YR, et al. Role of magnetic resonance imaging and apparent diffusion coefficient at 3T in distinguishing between adenocarcinoma of the uterine cervix and endometrium. Chang Gung Med J. 2011;34(1):93–100.
- Gui B, Lupinelli M, Russo L, et al. MRI in uterine cancers with uncertain origin: Endometrial or cervical? Radiological point of view with review of the literature. European journal of radiology. 2022;153:110357. doi: 10.1016/j.ejrad.2022.110357
- Tarachkova EV, Shorikov MA, Panov VO, et al. Possibilities of multiparametric MRI in the differential diagnosis of histological types of cervical cancer in the preoperative period. Tumors of female reproductive system. 2016;12(2):60–69. doi: 10.17650/1994-4098-2016-12-2-60-69
- Yemelyanova A, Vang R, Seidman JD, Gravitt PE, Ronnett BM. Endocervical adenocarcinomas with prominent endometrial or endomyometrial involvement simulating primary endometrial carcinomas: utility of HPV DNA detection and immunohistochemical expression of p16 and hormone receptors to confirm the cervical origin of the corpus tumor. Am J Surg Pathol. 2009;33(6):914–924. doi: 10.1097/PAS.0b013e3181971fdd
- Jain P, Aggarwal A, Ghasi RG, et al. Role of MRI in diagnosing the primary site of origin in indeterminate cases of uterocervical carcinomas: a systematic review and meta-analysis. Br J Radiol. 2022;95(1129):20210428. doi: 10.1259/bjr.20210428
补充文件






