

")


Comparison of multiparametric and biparametric magnetic resonance imaging protocols for prostate cancer diagnosis by radiologists with different experience
- Autores: Vasilev Y.A.1, Omelyanskaya O.V.1, Vladzymyrskyy A.V.1, Gelezhe P.B.1,2, Reshetnikov R.V.1, Gonchar A.P.1, Blokhin I.A.1, Abdullin I.I.1, Kieva I.N.3
-
Afiliações:
- Moscow Center for Diagnostics and Telemedicine
- Joint stock company “European Medical Center”
- Speransky Children’s Hospital
- Edição: Volume 4, Nº 4 (2023)
- Páginas: 455-466
- Seção: Original Study Articles
- URL: https://journals.rcsi.science/DD/article/view/262947
- DOI: https://doi.org/10.17816/DD322816
- ID: 262947
Citar

Resumo
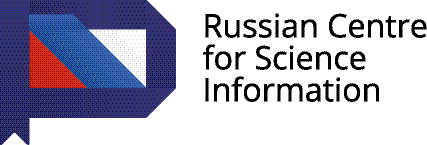
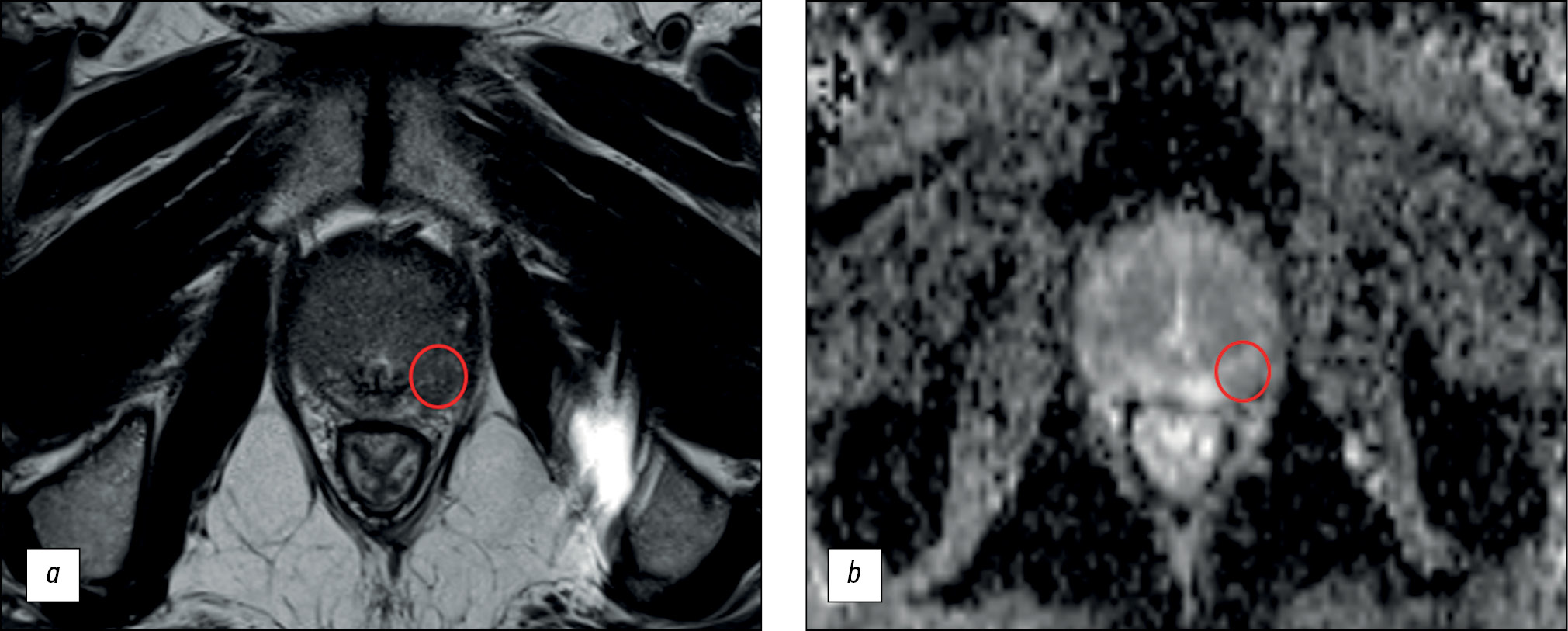
BACKGROUND: Magnetic resonance imaging can detect clinically significant prostate cancer and diagnose extracapsular extension and cancer stage. A scanning protocol that includes only T2-weighted and diffusion-weighted images represents a viable alternative to multiparametric magnetic resonance imaging provided that the high diagnostic accuracy of the test is maintained. In recent studies, biparametric and multiparametric magnetic resonance imaging demonstrated slight differences in the diagnostic accuracy in detecting prostate cancer.
AIM: To compare the diagnostic accuracy of biparametric and multiparametric magnetic resonance imaging for the detection of clinically significant prostate cancer using PI-RADS v2.1 with magnetic resonance imaging-guided multifocal biopsy as the gold standard.
MATERIALS AND METHODS: This retrospective study initially processed the medical records of 126 patients. The inclusion criteria were as follows: presence of PI-RADS 2.1 multiparametric magnetic resonance imaging, clinical information on free and bound prostate-specific antigen blood levels, a multifocal prostate biopsy performed, and a time interval between magnetic resonance imaging and biopsy of no more than 14 days. Three investigators (radiologists with <2, 2–5, and >5 years of experience) independently evaluated biparametric magnetic resonance imaging of the prostate for the presence of pathological foci. After 2 weeks, the researchers evaluated the multiparametric magnetic resonance imaging dataset of the prostate. Each lesion detected, starting from PI-RADS category 3, was compared with the result of a multifocal fusion biopsy. The biopsy result was presented as a sum of Gleason scores, and a Gleason score of ≥7 was considered clinically relevant. According to magnetic resonance imaging data, findings meeting PI-RADS criteria 4 and 5 were considered tumor foci.
RESULTS: The best values of sensitivity and specificity of foci detection on magnetic resonance imaging of the prostate gland were 62.5% and 74.6%, respectively. The highest diagnostic accuracy achieved was 70.1%. Magnetic resonance imaging had higher specificity rates for detecting prostatic foci when interpreted by radiologists with 2 years and >5 years of experience.
CONCLUSION: Both biparametric and multiparametric magnetic resonance imaging of the prostate demonstrated suboptimal diagnostic accuracy. The sensitivity and specificity of the method tended to improve with increasing experience of the radiologist. Biparametric protocols of prostate scanning have a definite economic advantage over multiparametric protocols because of the absence of contrast agents and consumables and a significant decrease in magnetic resonance scanner loading time; however, their use can lead to a decrease in the diagnostic accuracy of the method.
Palavras-chave
Texto integral
##article.viewOnOriginalSite##Sobre autores
Yuriy Vasilev
Moscow Center for Diagnostics and Telemedicine
Email: npcmr@zdrav.mos.ru
ORCID ID: 0000-0002-0208-5218
Código SPIN: 4458-5608
MD, Cand. Sci. (Med)
Rússia, MoscowOlga Omelyanskaya
Moscow Center for Diagnostics and Telemedicine
Email: o.omelyanskaya@npcmr.ru
ORCID ID: 0000-0002-0245-4431
Código SPIN: 8948-6152
Rússia, Moscow
Anton Vladzymyrskyy
Moscow Center for Diagnostics and Telemedicine
Email: npcmr@zdrav.mos.ru
ORCID ID: 0000-0002-2990-7736
Código SPIN: 3602-7120
MD, Dr. Sci. (Med), Professor
Rússia, MoscowPavel Gelezhe
Moscow Center for Diagnostics and Telemedicine; Joint stock company “European Medical Center”
Autor responsável pela correspondência
Email: gelezhe.pavel@gmail.com
ORCID ID: 0000-0003-1072-2202
Código SPIN: 4841-3234
Rússia, Moscow; Moscow
Roman Reshetnikov
Moscow Center for Diagnostics and Telemedicine
Email: reshetnikov@fbb.msu.ru
ORCID ID: 0000-0002-9661-0254
Código SPIN: 8592-0558
Rússia, Moscow
Anna Gonchar
Moscow Center for Diagnostics and Telemedicine
Email: a.gonchar@npcmr.ru
ORCID ID: 0000-0001-5161-6540
Código SPIN: 3513-9531
Rússia, Moscow
Ivan Blokhin
Moscow Center for Diagnostics and Telemedicine
Email: i.blokhin@npcmr.ru
ORCID ID: 0000-0002-2681-9378
Código SPIN: 3306-1387
Rússia, Moscow
Iskander Abdullin
Moscow Center for Diagnostics and Telemedicine
Email: iabdullin@emcmos.ru
ORCID ID: 0000-0003-1138-0822
Código SPIN: 6560-5219
Rússia, Moscow
Irina Kieva
Speransky Children’s Hospital
Email: kieva.irina@gmail.com
ORCID ID: 0000-0002-4060-5966
Código SPIN: 2279-9141
Rússia, Moscow
Bibliografia
- Turkbey B, Rosenkrantz AB, Haider MA, et al. Prostate imaging reporting and data system version 2.1: 2019 Update of prostate imaging reporting and data system version 2. Eur Urol. 2019;76(3):340–351. doi: 10.1016/j.eururo.2019.02.0331
- Bjurlin MA, Carroll PR, Eggener S, et al. Update of the standard operating procedure on the use of multiparametric magnetic resonance imaging for the diagnosis, staging and management of prostate cancer. J Urol. 2020;203(4):706–712. doi: 10.1097/JU.0000000000000617
- Rouvière O, Puech P, Renard-Penna R, et al. Use of prostate systematic and targeted biopsy on the basis of multiparametric MRI in biopsy-naive patients (MRI-FIRST): A prospective, multicentre, paired diagnostic study. Lancet Oncology. 2019;20(1):100–109. doi: 10.1016/S1470-2045(18)30569-2
- Boesen L, Thomsen FB, Nørgaard N, et al. A predictive model based on biparametric magnetic resonance imaging and clinical parameters for improved risk assessment and selection of biopsy-naïve men for prostate biopsies. Prostate Cancer Prostatic Dis. 2019;22(4):609–616. doi: 10.1038/s41391-019-0149-y
- Tamada T, Kido A, Yamamoto A, et al. Comparison of biparametric and multiparametric MRI for clinically significant prostate cancer detection with PI-RADS Version 2.1. J Magnetic Resonance Imaging. 2021;53(1):283–291. doi: 10.1002/jmri.27283
- Wallström J, Geterud K, Kohestani K, et al. Bi- or multiparametric MRI in a sequential screening program for prostate cancer with PSA followed by MRI? Results from the Göteborg prostate cancer screening 2 trial. Eur Radiol. 2021;31(11):8692–8702. doi: 10.1007/s00330-021-07907-9
- Kuhl CK, Bruhn R, Krämer N, et al. Abbreviated biparametric prostate MR imaging in men with elevated prostate-specific antigen. Radiology. 2017;285(2):493–505. doi: 10.1148/radiol.2017170129
- Abuladze LR, Semenov DS, Panina OV, Vasil AA. Optimized protocol of biparametric magnetic resonance imaging for prostate. Digital Diagnostics. 2022;3(3):166–177. doi: 10.17816/DD108484
- Schoots IG, Barentsz JO, Bittencourt LK, et al. PI-RADS committee position on MRI without contrast medium in biopsy-naive men with suspected prostate cancer: Narrative review. Am J Roentgenol. 2021;216(1):3–19. doi: 10.2214/AJR.20.24268
- Gleason DF. Classification of prostatic carcinomas. Cancer Chemother Rep. 1966;50(3):125–128.
- Zawaideh JP, Sala E, Shaida N, et al. Diagnostic accuracy of biparametric versus multiparametric prostate MRI: Assessment of contrast benefit in clinical practice. Eur Radiol. 2020;30(7):4039–4049. doi: 10.1007/s00330-020-06782-0
- Kang Z, Min X, Weinreb J, et al. Abbreviated biparametric versus standard multiparametric MRI for diagnosis of prostate cancer: A systematic review and meta-analysis. Am J Roentgenol. 2019;212(2):357–365. doi: 10.2214/AJR.18.20103
- Niu XK, Chen XH, Chen ZF, et al. Diagnostic performance of biparametric MRI for detection of prostate cancer: A systematic review and meta-analysis. Am J Roentgenol. 2018;211(2):369–378. doi: 10.2214/AJR.17.18946
- Ahmed HU, El-Shater Bosaily A, Brown LC, et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet. 2017;389(10071):815–822. doi: 10.1016/S0140-6736(16)32401-1
- McDonald RJ, Levine D, Weinreb J, et al. Gadolinium retention: A research roadmap from the 2018 NIH/ACR/RSNA workshop on gadolinium chelates. Radiology. 2018;289(2):517–534. doi: 10.1148/radiol.2018181151
- Ploussard G, Epstein JI, Montironi R, et al. The contemporary concept of significant versus insignificant prostate cancer. Eur Urol. 2011;60(2):291–303. doi: 10.1016/j.eururo.2011.05.006
- Loeb S, Vellekoop A, Ahmed HU, et al. Systematic review of complications of prostate biopsy. Eur Urol. 2013;64(6):876–892. doi: 10.1016/j.eururo.2013.05.049
- Campli ED, Pizzi DA, Seccia B, et al. Diagnostic accuracy of biparametric vs multiparametric MRI in clinically significant prostate cancer: Comparison between readers with different experience. Eur J Radiol. 2018;(101):17–23. doi: 10.1016/j.ejrad.2018.01.028
- Gatti M, Faletti R, Calleris G, et al. Prostate cancer detection with biparametric magnetic resonance imaging (bpMRI) by readers with different experience: Performance and comparison with multiparametric (mpMRI). Abdominal Radiol (New York). 2019;44(5):1883–1893. doi: 10.1007/s00261-019-01934-3
Arquivos suplementares



