

")



糖皮质激素治疗新型冠状病毒感染罕见局限性缺血性坏死
- 作者: Gonchar A.P.1, Blokhin I.A.1, Shumskaya Y.F.1,2
-
隶属关系:
- Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
- The First Sechenov Moscow State Medical University (Sechenov University)
- 期: 卷 3, 编号 4 (2022)
- 页面: 384-392
- 栏目: 临床病例及临床病例的系列
- URL: https://journals.rcsi.science/DD/article/view/146867
- DOI: https://doi.org/10.17816/DD110718
- ID: 146867
如何引用文章

详细
糖皮质激素治疗新型冠状病毒感染引起的骨结构缺血性坏死是一种相当常见的治疗并发症,其中最常见的是股骨头病变。对于预防关节炎和其他并发症,及时检测缺血性坏死是很重要的。
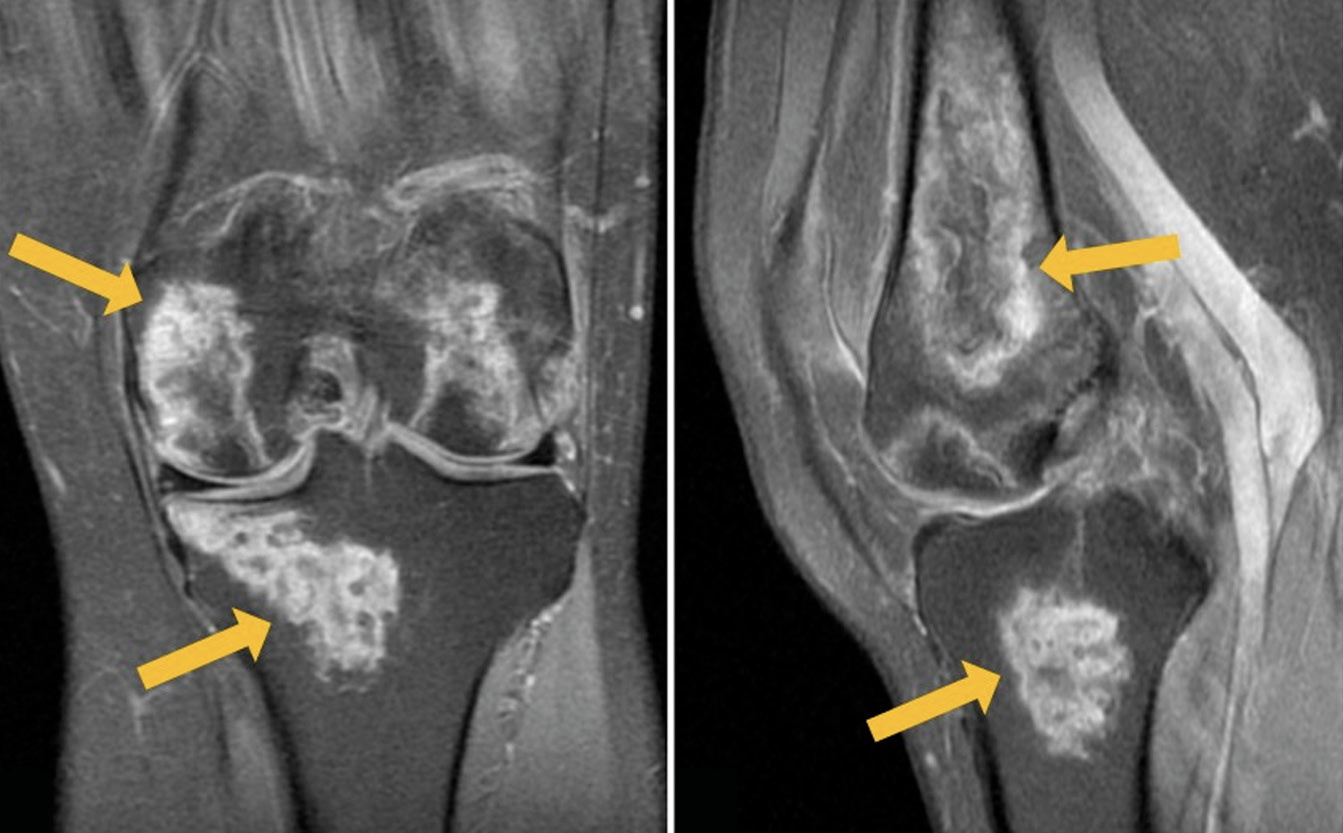
这项研究展示了一名54岁的患者的临床案例,她因新冠状病毒感染住院,并在发病后两周内抱怨双膝关节疼痛。磁共振成像扫描显示,形成膝关节的骨骼在两侧都有明显的血管性坏死。使用非甾体抗炎药和双磷酸盐骨吸收抑制剂的保守治疗有显著的积极效果。3个月后复查时,没有疼痛,但膝关节的活动仍有轻微限制。两个膝关节的磁共振成像显示,先前确定的变化明显减少。
糖皮质激素的副作用(糖耐量受损、血压升高、心动过速、胃肠道侵蚀性溃疡、睡眠障碍等)广为人知,但由类固醇引起的膝关节骨结构的骨坏死却很少引起临床医生的注意。这个临床病例强调了骨坏死发病机制的复杂性,并展示了皮质类固醇治疗的广泛并发症。
作者简介
Anna P. Gonchar
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
Email: a.gonchar@npcmr.ru
ORCID iD: 0000-0001-5161-6540
SPIN 代码: 3513-9531
俄罗斯联邦, Moscow
Ivan A. Blokhin
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
Email: i.blokhin@npcmr.ru
ORCID iD: 0000-0002-2681-9378
SPIN 代码: 3306-1387
俄罗斯联邦, Moscow
Yuliya F. Shumskaya
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies; The First Sechenov Moscow State Medical University (Sechenov University)
编辑信件的主要联系方式.
Email: yu.shumskaia@npcmr.ru
ORCID iD: 0000-0002-8521-4045
SPIN 代码: 3164-5518
俄罗斯联邦, Moscow; Moscow
参考
- Temporary guidelines «Prevention, diagnosis and treatment of new coronavirus infection (COVID-19)». Version 3 (March 3, 2020) (approved by the Ministry of Health of the Russian Federation). (In Russ). Available from: https://www.garant.ru/products/ipo/prime/doc/73647088/. Accessed: 15.07.2022.
- Ali RS, Al-Sudani H, Tan IJ. Osteonecrosis of bilateral distal femurs in a pregnant patient following antenatal betamethasone. Cureus. 2022;14(3):e22735. doi: 10.7759/cureus.22735
- Zhang S, Wang C, Shi L, Xue Q. Beware of steroid-induced avascular necrosis of the femoral head in the treatment of COVID-19-experience and lessons from the SARS epidemic. Drug Des Devel Ther. 2021;15:983–995. doi: 10.2147/DDDT.S298691
- Agarwala SR, Vijayvargiya M, Pandey P. Avascular necrosis as a part of ‘long COVID-19’. BMJ Case Rep. 2021;14(7):e242101. doi: 10.1136/bcr-2021-242101
- Takao M, Sugano N, Nishii T, et al. Spontaneous regression of steroid-related osteonecrosis of the knee. Clin Orthop Relat Res. 2006;452:210–215. doi: 10.1097/01.blo.0000229278.51323.08
- Hines JT, Jo WL, Cui Q, et al. Osteonecrosis of the femoral head: an updated review of arco on pathogenesis, staging and treatment. J Korean Med Sci. 2021;36(24):e177. doi: 10.3346/jkms.2021.36.e177
- Disser NP, De Micheli AJ, Schonk MM, et al. Musculoskeletal consequences of COVID-19. J Bone Joint Surg Am. 2020;102(14):1197–1204. doi: 10.2106/JBJS.20.00847
- Karim AR, Cherian JJ, Jauregui JJ, et al. Osteonecrosis of the knee: review. Ann Transl Med. 2015;3(1):6. doi: 10.3978/j.issn.2305-5839.2014.11.13
- Patel MS, Gutman MJ, Abboud JA. Orthopaedic considerations following COVID-19: lessons from the 2003 SARS outbreak. JBJS Rev. 2020;8(7):e2000052. doi: 10.2106/JBJS.RVW.20.00052
- Kerachian MA, Séguin C, Harvey EJ. Glucocorticoids in osteonecrosis of the femoral head: a new understanding of the mechanisms of action. J Steroid Biochem Mol Biol. 2009;114(3-5):121–128. doi: 10.1016/j.jsbmb.2009.02.007
- Chan KL, Mok CC. Glucocorticoid-induced avascular bone necrosis: diagnosis and management. Open Orthop J. 2012;6:449–457. doi: 10.2174/1874325001206010449
- Powell C, Chang C, Naguwa SM, et al. Steroid induced osteonecrosis: an analysis of steroid dosing risk. Autoimmun Rev. 2010;9(11):721–743. doi: 10.1016/j.autrev.2010.06.007
- Takeda H, Nishise S, Fujishima S, et al. Osteonecrosis of the lateral femoral condyle in a patient with ulcerative colitis: report of a case. Clin J Gastroenterol. 2008;1(3):93–96. doi: 10.1007/s12328-008-0015-2
- Agarwala SR, Vijayvargiya M, Sawant T. Secondary osteonecrosis of the knee as a part of long COVID-19 syndrome: a case series. BMJ Case Rep. 2022;15(3):e248583. doi: 10.1136/bcr-2021-248583
- Angulo-Ardoy M, Ureña-Aguilera Á. Knee osteonecrosis after COVID-19. Fam Pract. 2021;38(Suppl 1):i45–i47. doi: 10.1093/fampra/cmab063
- Sulewski A, Sieroń D, Szyluk K, et al. Avascular necrosis bone complication after active COVID-19 infection: preliminary results. Medicina (Kaunas). 2021;57(12):1311. doi: 10.3390/medicina57121311
- Li W, Huang Z, Tan B, et al. General recommendation for assessment and management on the risk of glucocorticoid-induced osteonecrosis in patients with COVID-19. J Orthop Translat. 2021;31:1–9. doi: 10.1016/j.jot.2021.09.005
- Mont MA, Baumgarten KM, Rifai A, et al. Atraumatic osteonecrosis of the knee. J Bone Joint Surg Am. 2000;82(9):1279–1290. doi: 10.2106/00004623-200009000-00008
- Agarwala S, Sharoff L, Jagani N. Effect of zoledronic acid and alendronate on bone edema and pain in spontaneous osteonecrosis of the knee: a new paradigm in the medical management. Rev Bras Ortop (Sao Paulo). 2020;55(5):543–550. doi: 10.1016/j.rboe.2017.12.008
- Jureus J, Lindstrand A, Geijer M, et al. Treatment of spontaneous osteonecrosis of the knee (SPONK) by a bisphosphonate. Acta Orthop. 2012;83(5):511–514. doi: 10.3109/17453674.2012.729184
补充文件





