

")



Substantiation of a new approach to the criteria for assessing the radiation dose of patients during computed tomography
- Authors: Matkevich E.I.1,2, Sinitsyn V.Е.2,3, Ivanov I.V.4,5
-
Affiliations:
- State Research Center - Burnasyan Federal Medical Biophysical Center of Federal Medical Biological Agency
- I.V. Davydovsky City Clinical Hospital
- Lomonosov Moscow State University
- Sechenov First Moscow State Medical University (Sechenov University)
- State Scientific-Research Test Institute of Military Medicine
- Issue: Vol 3, No 4 (2022)
- Pages: 344-361
- Section: Original Study Articles
- URL: https://journals.rcsi.science/DD/article/view/146864
- DOI: https://doi.org/10.17816/DD110857
- ID: 146864
Cite item

Abstract
BACKGROUND: In accordance with the requirements of the IAEA basic safety standards and the International Commission on Radiation Protection, comparing the radiation dose for patients undergoing computed tomography (CT) in diagnostic and treatment clinics with national or international DRLs is important for controlling medical radiation doses. The search for ways to improve DRLs calculations determines the relevance of such studies.
AIM: To analyze the dependence of effective doses (EDs) in CT of different body parts on patient’s weight and to calculate the standard ED for the patient (70 and 80 kg).
MATERIALS AND METHODS: CT acquisition protocols in 209 patients were single phase (SP) CT, while 114 patients underwent multi-phase (MP) CT. ED was calculated according to the normalized coefficients for each body area. The values of standard ED was calculated by data approximation using linear function of ED relatively body weight for each type CT scanner and body area scanned.
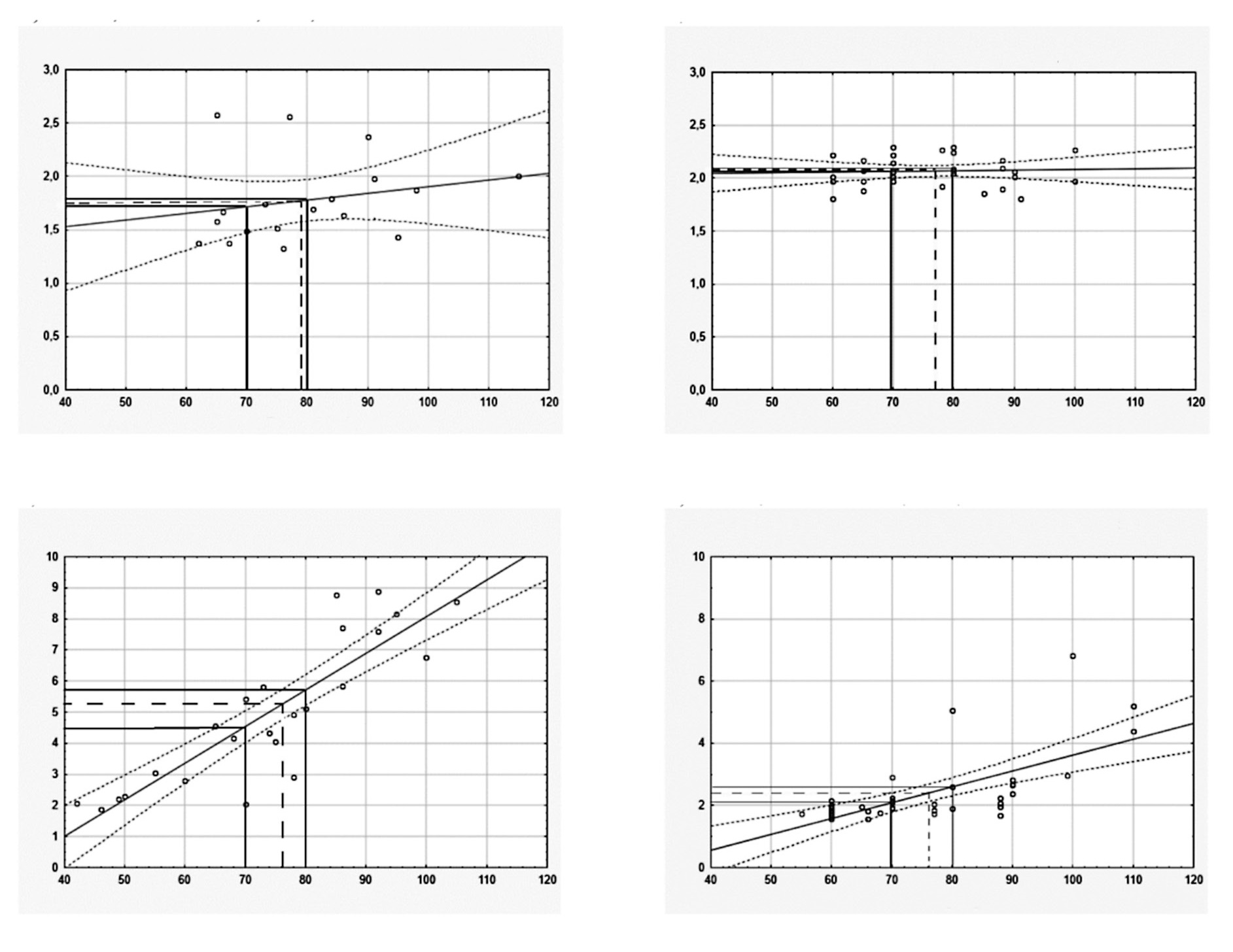
RESULTS: The increase in ED following a CT examination was proportional to the body weight of patients. For SP and MP CT scans, the standard EDs were calculated according to all body areas. The mean ED, median ED, and DRLs (mSv) in these groups was slightly higher than standard ED (mSv) if the criterion was 70 kg and were close to standard ED if the criterion was 80 kg. These values give a basis for improving the guidelines concerning the recommended limits of radiation doses for CT in individual patients according to indications and body parts studied.
CONCLUSIONS: In the study, a methodology for assessing and comparing the dose of CT-radiation at two hospitals in the two CT scanners, considering weight of a standard patient, is described. Our results show that the calculation and analysis of the standard ED of CT-examining areas of the body instead of mean ED and median ED help to compare the radiation exposure in different medical facilities more properly. Given the recent sharp increase in the number of CT studies, not exceeding the standard ED for patients with CT will reduce the long-term consequences in the form of oncological pathology among the population.
Full Text
##article.viewOnOriginalSite##About the authors
Elena I. Matkevich
State Research Center - Burnasyan Federal Medical Biophysical Center of Federal Medical Biological Agency; I.V. Davydovsky City Clinical Hospital
Email: pencil_red@mail.ru
ORCID iD: 0000-0001-5917-7706
SPIN-code: 5546-4830
MD, Cand. Sci. (Med.)
Russian Federation, Moscow; MoscowValentin Е. Sinitsyn
I.V. Davydovsky City Clinical Hospital; Lomonosov Moscow State University
Email: vsini@mail.ru
ORCID iD: 0000-0002-5649-2193
SPIN-code: 8449-6590
MD, Dr. Sci. (Med.), Professor
Russian Federation, Moscow; MoscowIvan V. Ivanov
Sechenov First Moscow State Medical University (Sechenov University); State Scientific-Research Test Institute of Military Medicine
Author for correspondence.
Email: ivanov-iv@yandex.ru
ORCID iD: 0000-0001-7729-2724
SPIN-code: 9888-2780
MD, Dr. Sci. (Med.), Professor
Russian Federation, Moscow; Saint PetersburgReferences
- On the state of sanitary and epidemiological welfare of the population in the Russian Federation in 2021. State report. Available from: https://www.rospotrebnadzor.ru/documents/details.php?ELEMENT_ID=21796. Accessed: 25.10.2022.
- IAEA [Internet]. Radiation Protection and Safety of Radiation Sources: International Basic Safety Standards, IAEA Safety Standards Series No. GSR Part 3. IAEA, Vienna, 2014. Available from: https://www.iaea.org/publications/8930/radiation-protection-and-safety-of-radiation-sources-international-basic-safety-standards. Accessed: 25.10.2022.
- Recommendations of the International Commission on Radiological Protection. Ann ICRP. 1991;21(1-3):1–201.
- EUR16262 [Internet]. European guidelines on quality criteria in Computed Tomography. Brussels, Belgium: European Commission, Report EUR 16262. 1999. Available from: https://op.europa.eu/da/publication-detail/-/publication/d229c9e1-a967-49de-b169-59ee68605f1a. Accessed: 25.10.2022.
- The 2007 Recommendations of the International Commission on Radiological Protection. ICRP publication 103. Ann ICRP. 2007;37(2-4):1–332. doi: 10.1016/j.icrp.2007.10.003
- Radiation protection in medicine. ICRP Publication 105. Ann ICRP. 2007;37(6):1–63. doi: 10.1016/j.icrp.2008.08.001.
- Diagnostic reference levels in medical imaging. ICRP Publication 135. Ann ICRP. 2017;46(1):1–144. doi: 10.1177/0146645317717209
- Prokop M, Galanski M. Spiral and multislice computed tomography of the body. Vol. 2. Germany: Stuttgard, Verlag KG, cop. 2002.
- Monitoring of the effective doses of patient due to medical x-ray examinations. Changes in Methodical guidelines MU 2.6.1.2944-11. 2.6.1. Ionizing radiation, radiation safety. Available from: https://www.rospotrebnadzor.ru/upload/iblock/71e/mu-2.6.1.3584_19-izmeneniya-v-mu-2.6.1.2944_11.pdf. Accessed: 25.10.2022.
- The application of reference diagnostic levels for optimization of patient’s radiation protection during X-ray examinations of general purpose. Methodological recommendations MR 2.6.1.0066-12. Available from: https://rospotrebnadzor.ru/documents/details.php?ELEMENT_ID=4656. Accessed: 25.10.2022.
- Hinrichs RN. Adjustments to the segment center of mass proportions of Clauser et al. (1969). J Biomech. 1990;23(9):949–951. doi: 10.1016/0021-9290(90)90361-6
- Dubrovsky VI, Fedorova VN. Biomechanics: Textbook. For secondary and higher educational institutions. Moscow: VLADOS-PRESS; 2003. 550 p.
- Ozlib.com [Internet]. Common center of mass, common center of gravity, geometry of masses, anthropometry. In: Biomechanics. Knowledge of body-motor exercises. 2013. Available from: https://ozlib.com/801945/sport/obschiy_tsentr_mass_obschiy_tsentr_tyazhesti_geometriya_mass_antropometriya. Accessed: 25.10.2022.
- Helpiks.org [Internet]. Distribution of mass in the human body. Available from: https://helpiks.org/6-6110.html. Accessed: 25.10.2022.
- Garba I, Zarb F, McEntee MF, Fabri SG. Computed tomography diagnostic reference levels for adult brain, chest and abdominal examinations: a systematic review. Radiography (Lond). 2021;27(2):673–681. doi: 10.1016/j.radi.2020.08.011
- Smith-Bindman R, Wang Y, Yellen-Nelson TR, et al. Predictors of CT radiation dose and their effect on patient care: a comprehensive analysis using automated data. Radiology. 2017;282(1):182–193. doi: 10.1148/radiol.2016151391
- Smith-Bindman R, Wang Y, Chu P, et al. International variation in radiation dose for computed tomography examinations: prospective cohort study. BMJ. 2019;(364):k4931. doi: 10.1136/bmj.k4931
- Van der Molen AJ, Schilham A, Stoop P, et al. A national survey on radiation dose in CT in The Netherlands. Insights Imaging. 2013;4(3):383–390. doi: 10.1007/s13244-013-0253-9
- Al Naemi H, Tsapaki V, Omar AJ, et al. Towards establishment of diagnostic reference levels based on clinical indication in the state of Qatar. Eur J Radiol Open. 2020;7:100282. doi: 10.1016/j.ejro.2020.100282
- Heggie JC. Patient doses in multi-slice CT and the importance of optimisation. Australas Phys Eng Sci Med. 2005;28(2):86–96. doi: 10.1007/BF03178698
- Rivers-Bowerman MD, Shiva Shankar JJ. Iterative reconstruction for head CT: Effects on radiation dose and image quality. Can J Neurol Sci. 2014;41(5):620–625. doi: 10.1017/cjn.2014.11
- MacGregor K, Li I, Dowdell T, Gray BG. Identifying institutional diagnostic reference levels for CT with radiation dose index monitoring software. Radiology. 2015;276(2):507–517. doi: 10.1148/radiol.2015141520
- IAEA-TECDOC-1621 [Internet]. Dose Reduction in CT while Maintaining Diagnostic Confidence: A Feasibility/Demonstration Study. IAEA, Vienna; 2009. Available from: https://www-pub.iaea.org/MTCD/Publications/PDF/te_1621_web.pdf. Accessed: 25.10.2022.
- Qi LP, Li Y, Tang L, Li YL, et al. Evaluation of dose reduction and image quality in chest CT using adaptive statistical iterative reconstruction with the same group of patients. Br J Radiol. 2012;85(1018):e906–e911. doi: 10.1259/bjr/66327067
- Yasaka K, Katsura M, Akahane M, et al. Model-based iterative reconstruction for reduction of radiation dose in abdominopelvic CT: Comparison to adaptive statistical iterative reconstruction. Springerplus. 2013;2(1):209. doi: 10.1186/2193-1801-2-209
- Hofer M. CT teaching manual: a systematic approach to CT reading. Thieme; 2005. 208 p.
- Tsapaki V, Aldrich JE, Sharma R, et al. Dose reduction in CT while maintaining diagnostic confidence: Diagnostic reference levels at routine head, chest, and abdominal CT-IAEA-coordinated research project. Radiology. 2006;240(3):828–834. doi: 10.1148/radiol.2403050993
- Calderoni F, Campanaro F, Colombo PE, et al. Analysis of a multicentre cloud-based CT dosimetric database: Preliminary results. Eur Radiol Exp. 2019;3(1):27. doi: 10.1186/s41747-019-0105-6
- Shin HJ, Chung YE, Lee YH, et al. Radiation dose reduction via sinogram affirmed iterative reconstruction and automatic tube voltage modulation (CARE kV) in abdominal CT. Korean J Radiol. 2013;14(6):886–893. doi: 10.3348/kjr.2013.14.6.886
- Kim K, Kim YH, Kim SY, et al. Low-dose abdominal CT for evaluating suspected appendicitis. N Engl J Med. 2012;366(17):1596–1605. doi: 10.1056/NEJMoa1110734
- Abuzaid MM, Elshami W, Tekin HO et al. Computed tomography radiation doses for common computed tomography examinations: a nationwide dose survey in United Arab Emirates. Insights Imaging 11, 88 (2020). https://doi.org/10.1186/s13244-020-00891-6
- Shrimpton PC, Hillier MC, Lewis MA, Dunn M. National survey of doses from CT in the UK: 2003. Br J Radiol. 2006;79(948):968–980. doi: 10.1259/bjr/93277434
- Mettler F, Huda W, Yoshizumi T, Mahesh M. Effective doses in radiology and diagnostic nuclear medicine: A catalog. Radiology. 2008;248(1):254–263. doi: 10.1148/radiol.2481071451
- Pickhardt PJ, Lubner MG, Kim DH, et al. Abdominal CT with model-based iterative reconstruction (MBIR): Initial results of a prospective trial comparing ultralow-dose with standard-dose imaging. Am J Roentgenol. 2012;199(6):1266–1274. doi: 10.2214/AJR.12.9382
- Zewdu M, Kadir E, Tesfaye M, Berhane M. Establishing local diagnostic reference levels for routine computed tomography examinations in JIMMA university medical center south West Ethiopia. Radiat Prot Dosimetry. 2021;193(3-4):200–206. doi: 10.1093/rpd/ncab028
- Atlı E, Uyanık SA, Öğüşlü U, et al. Radiation doses from head, neck, chest and abdominal CT examinations: An institutional dose report. Diagn Interv Radiol. 2021;27(1):147–151. doi: 10.5152/dir.2020.19560
- Brat H, Zanca F, Montandon S, et al. Local clinical diagnostic reference levels for chest and abdomen CT examinations in adults as a function of body mass index and clinical indication: A prospective multicenter study. Eur Radiol. 2019;29(12):6794–6804. doi: 10.1007/s00330-019-06257-x
- Hu X, Gou J, Lin W, et al. Size-specific dose estimates of adult, chest computed tomography examinations: Comparison of Chinese and updated 2017 American College of Radiology diagnostic reference levels based on the water-equivalent diameter. PLoS One. 2021;16(9):e0257294. doi: 10.1371/journal.pone.0257294
- Li X, Steigerwalt D, Rehani M. T-shirt size as a classification for body habitus in computed tomography (CT) and development of size-based dose reference levels for different indications. Eur J Radiol. 2022;151(3):110289. doi: 10.1016/j.ejrad.2022.110289
- Westra SJ, Li X, Gulat K, et al. Entrance skin dosimetry and size-specific dose estimatefrom pediatric chest CTA. J Cardiovasc Comput Tomogr. 2014;8(2):97–107. doi: 10.1016/j.jcct.2013.08.002
- Strauss KJ. CT: Size Specific Dose Estimate (SSDE): Why We Need Another CT Dose Index. Clinical Imaging Physicist Cincinnati Children’s Hospital University of Cincinnati College of Medicine. In: Boone J, McCollough C, McNitt-Grey M, et al. Acknowledgements. Available from: https://docplayer.net/20784880-Ct-size-specific-dose-estimate-ssde-why-we-need-another-ct-dose-index-acknowledgements.html. Accessed: 25.10.2022.
- Özsoykal İ, Yurt A, Akgüngör K. Size-specific dose estimates in chest, abdomen, and pelvis CT examinations of pediatric patients. Diagn Interv Radiol. 2018;24(4):243–248. doi: 10.5152/dir.2018.17450
- Lyra M, Rouchota M, Michalitsi M, Boultadaki A. Effective dose and size-specific dose estimate (SSDE) of the torso: In low dose MDCT protocol in multiple myeloma. Radiol Diagn Imaging. 2019. doi: 10.15761/RDI.1000146
- Matkevich EI, Sinitsyn VE, Ivanov IV. Health prediction indices obtained with low-dose computer tomography scans. Aviakosm Ekolog Med. 2015;49(6):61–67. (In Russ).
- The use of reference diagnostic levels for adult patients in radiation diagnostics. Methodological recommendations. Moscow; 2020. 38 р. (In Russ).
- Damilakis J, Vassileva J. The growing potential of diagnostic reference levels as a dynamic tool for dose optimization. Physica Medica. 2021;84:285–287. doi: 10.1016/j.ejmp.2021.03.018
- Moghadam N, Lecomte R, Mercure S, et al. Simplified size adjusted dose reference levels for adult CT examinations: A regional study. Eur J Radiol. 2021;142:109861. doi: 10.1016/j.ejrad.2021.109861
- Almén A, Guðjónsdóttir J, Heimland N, et al. Establishing paediatric diagnostic reference levels using reference curves: A feasibility study including conventional and CT examinations. Phys Med. 2021;87:65–72. doi: 10.1016/j.ejmp.2021.05.035
- Smith-Bindman R, Lipson J, Marcus R, et al. Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancer. Arch Intern Med. 2009;169(22):2078–2086. doi: 10.1001/archinternmed.2009.427
- Smith-Bindman R. Environmental causes of breast cancer and radiation from medical imaging: Findings from the institute of medicine report. Arch Intern Med. 2012;172(13):1023–1027. doi: 10.1001/archinternmed.2012.2329
- Linet MS, Slovis TL, Miller DL, et al. Cancer risks associated with external radiation from diagnostic imaging procedures. CA Cancer J Clin. 2012;62(2):75–100. doi: 10.3322/caac.21132
- Golikov VY, Vodovatov AV, Chipiga LA, Shatsky IG. Assessment of radiation risk in patients during medical research in the Russian Federation. Radiation hygiene. 2021;14(3):56–68. (In Russ). doi: 10.21514/1998-426X-2021-14-3-56-68
- Druzhinin YV, Ryzhov SA, Vodovatov AV, et al. The influence of COVID-19 on the dynamics of changes in the dose load on patients during computed tomography in medical organizations in Moscow. Digital Diagnostics. 2022;3(1):5–15. doi: 10.17816/DD87628
Supplementary files



