



On the issue of diagnosis and treatment of skin pseudolymphoma on the example of a clinical case
- Authors: Olisova O.Y.1, Snarskaya E.S.1, Teplyuk N.P.1, Varshavsky V.A.1, Zolotareva E.S.1, Makhmudi W.1
-
Affiliations:
- The First Sechenov Moscow State Medical University (Sechenov University)
- Issue: Vol 26, No 2 (2023)
- Pages: 105-118
- Section: DERMATO-ONCOLOGY
- URL: https://journals.rcsi.science/1560-9588/article/view/132600
- DOI: https://doi.org/10.17816/dv217710
- ID: 132600
Cite item

Abstract
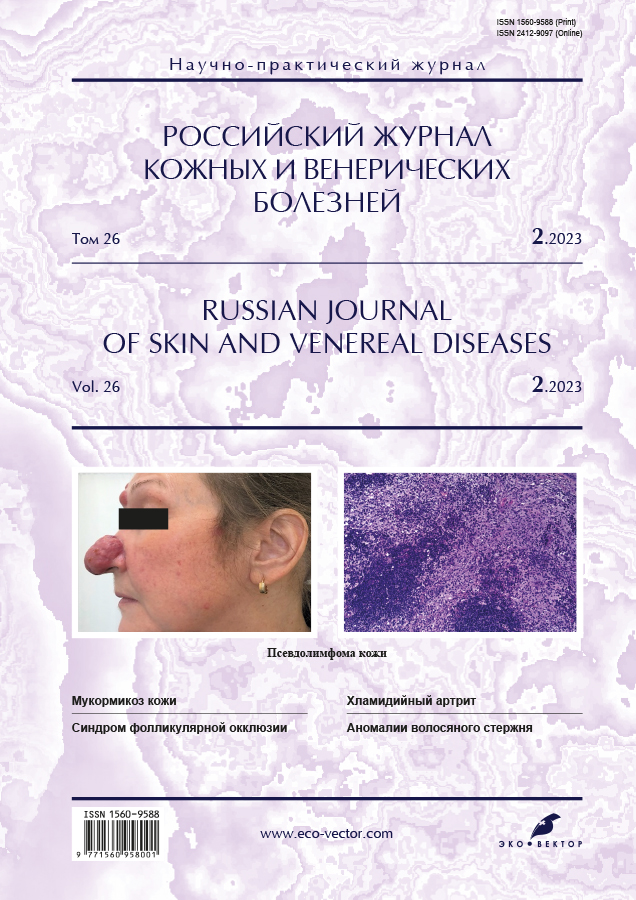
Pseudolymphomas of the skin are a heterogeneous group of diseases manifested by benign lymphoid infiltrates that clinically and/or histologically mimic skin lymphoma.
The group of pseudolymphomas of the skin includes actinic reticuloid, benign lymphocytoma of the skin, true pesvdolymphoma, postscabious lymphoplasia, lymphocytic reactions to insect bites, etc. The diagnosis of pseudolymphoma is based on anamnesis data (the presence of a provoking factor, with the exception of idiopathic pseudolymphomas), clinical picture (a single papule, less often a plaque localized in open areas of the upper half of the body ― the face: cheeks, nose, earlobes; scalp, upper extremities, chest), results histological, immunophenotypic studies, and with persistent persistence of rashes ― on the results of molecular biological studies.
The similarity of clinical and pathomorphological signs of pseudolymph with malignant lymphoproliferative processes creates significant diagnostic difficulties and requires a thorough examination with the involvement of pathologists and oncologists. Diagnostic difficulties are often the cause of erroneous or late detection of skin lymphoma, which negatively affects the prognosis of the disease. Treatment tactics are determined by the morphological variant of lymphoid infiltration, as well as the presence and nature of the provoking factor. The majority of idiopathic psvdolymph is successfully treated with systemic glucocorticosteroids, however, in the case of resistance to systemic glucocorticoids, recommendations on treatment tactics have not yet been developed. Prolonged, often recurrent course, as well as the possibility of transformation of the process into malignant lymphoma of the skin, requires long-term clinical observation of patients.
The case presented in the article confirms that the crucial importance for the successful diagnosis of pseudolymphoma lies in the analysis of anamnesis data, clinical picture, histological and immunohistochemical studies.
Full Text
##article.viewOnOriginalSite##About the authors
Olga Yu. Olisova
The First Sechenov Moscow State Medical University (Sechenov University)
Email: olisovaolga@mail.ru
ORCID iD: 0000-0003-2482-1754
SPIN-code: 2500-7989
MD, Dr. Sci. (Med.), Professor, Corresponding Member Russian Academy of Sciences
Russian Federation, 8-2 Trubetskaya street, 119992 MoscowElena S. Snarskaya
The First Sechenov Moscow State Medical University (Sechenov University)
Email: snarskaya-dok@mail.ru
ORCID iD: 0000-0002-7968-7663
SPIN-code: 3785-7859
MD, Dr. Sci. (Med.), Professor
Russian Federation, 8-2 Trubetskaya street, 119992 MoscowNatalya P. Teplyuk
The First Sechenov Moscow State Medical University (Sechenov University)
Email: teplyukn@gmail.com
ORCID iD: 0000-0002-5800-4800
SPIN-code: 8013-3256
MD, Dr. Sci. (Med.), professor
Russian Federation, 8-2 Trubetskaya street, 119992 MoscowVladimir A. Varshavsky
The First Sechenov Moscow State Medical University (Sechenov University)
Email: vavarsh@gmail.com
ORCID iD: 0000-0002-5855-3092
MD, Dr. Sci. (Med.), Proffessor
Russian Federation, 8-2 Trubetskaya street, 119992 MoscowEvgeniya S. Zolotareva
The First Sechenov Moscow State Medical University (Sechenov University)
Email: evgeniyazltrv@gmail.com
ORCID iD: 0000-0002-4086-1740
Clinical Resident of the Department of Skin and Venereal Diseases named after V.A. Rakhmanov
Russian Federation, 8-2 Trubetskaya street, 119992 MoscowWilliam Makhmudi
The First Sechenov Moscow State Medical University (Sechenov University)
Author for correspondence.
Email: dr.williamm@mail.ru
ORCID iD: 0000-0001-6075-411X
Russian Federation, 8-2 Trubetskaya street, 119992 Moscow
References
- Olisova OY, Potekaev NS. Pseudolymphomes of the skin. Moscow: Praktika; 2013. 138 p. (In Russ).
- Dermatooncology. Ed. by G.A. Galil-Ogly, V.A. Molochkov, Yu.V. Sergeev. Moscow: Meditsina dlya vsekh; 2005. P. 577–591. (In Russ).
- Olisova OY. Differential diagnosis of pseudolymph skin with localization on the face. Plastic Sur Cosmetol. 2011;(3):477–481. (In Russ).
- Shetty SK, Hegde U, Jagadish L, Shetty C. Pseudolymphoma versus lymphoma: An important diagnostic decision. J Oral Maxillofac Pathol. 2016;20(2):328. doi: 10.4103/0973-029X.185909
- Hussein MR. Cutaneous pseudolymphomas: Inflammatory reactive proliferations. Expert Rev Hematol. 2013;6(6):713–733. doi: 10.1586/17474086.2013.845000
- Engin B, Songür A, Kutlubay Z, Serdaroğlu S. Lymphocytic infiltrations of face. Clin Dermatol. 2014;32(1):101–108. doi: 10.1016/j.clindermatol.2013.05.031
- Makhecha M, Singh T, Yadav T, Atawane M. Cutaneous pseudolymphoma secondary to facial thread lift procedure. Indian Dermatol Online J. 2019;10(3):322–324. doi: 10.4103/idoj.IDOJ_166_18
- Lewin JM, Farley-Loftus R, Pomeranz MK. Herpes simplex virus-associated pseudolymphoma. Cutis. 2013;92(6):E1–2.
- Sepaskhah M, Yazdanpanah N, Sari AF, Jahromi AM. Cutaneous pseudolymphoma as a rare adverse effect of medicinal leech therapy: A case report and review of the literature. Cureus. 2020;12(4):e7517. doi: 10.7759/cureus.7517
- Maraspin V, Strle F. Borrelial lymphocytoma. Wien Klin Wochenschr. 2022. doi: 10.1007/s00508-022-02064-5
- Kendel M, Toncic RJ, Bradamante M, et al. Dermoscopy of a tattoo pseudolymphoma. Dermatol Pract Concept. 2019;9(1):17–19. doi: 10.5826/dpc.0901a04
- Riyaz N, Sasidharanpillai S, Aravindan KP, et al. Phenytoin induced cutaneous B cell pseudolymphoma. Indian J Dermatol. 2015;60(5):522. doi: 10.4103/0019-5154.164437
- Imafuku S, Ito K, Nakayama J. Cutaneous pseudolymphoma induced by adalimumab and reproduced by infliximab in a patient with arthropathic psoriasis. Br J Dermatol. 2012;166(3):675–678. doi: 10.1111/j.1365-2133.2011.10607.x
- Foley C, Leonard N, Wynne B. Cutaneous pseudolymphoma: A rare side effect of cyclosporine. J Am Acad Dermatol. 2015;72(3):e85–86. doi: 10.1016/j.jaad.2014.09.008
- Kim H, Lim KY, Kang J, et al. Macrophagic myofasciitis and subcutaneous pseudolymphoma caused by aluminium adjuvants. Sci Rep. 2020;10(1):11834. doi: 10.1038/s41598-020-68849-8
- Mintoff D, Scerri L, Betts A. SARS-CoV-2 mRNA vaccine injection site pseudolymphoma. J Eur Acad Dermatol Venereol. 2022;36(1):e20–e22. doi: 10.1111/jdv.17680
- Egawa G, Kabashima K. Role of lymphoid structure in skin immunity. Curr Top Microbiol Immunol. 2020;(426):65–82. doi: 10.1007/82_2020_206
- Ebrahim AS, Sabbagh H, Liddane A, et al. Hematologic malignancies: Newer strategies to counter the BCL-2 protein. J Cancer Res Clin Oncol. 2016;142(9):2013–2022. doi: 10.1007/s00432-016-2144-1
- Aslani SF, Sepaskhah M, Safaei A, Hormozi JS. Cutaneous pseudolymphoma: A clinicopathological study and immunohistochemical patterns. Caspian J Intern Med. 2021;12(3):283–289. doi: 10.22088/cjim.12.3.283
- Sidiropoulos M, Deonizio J, Martinez-Escala ME, et al. Chronic actinic dermatitis/actinic reticuloid: A clinicopathologic and immunohistochemical analysis of 37 cases. Am J Dermatopathol. 2014;36(11):875–881. doi: 10.1097/DAD.0000000000000076
- Tian Z, Shiyu Z, Tao W, et al. Lymphoma or pseudolymphoma: A report of six cases and review of the literature. Dermatol Ther. 2019;32(4):e12807. doi: 10.1111/dth.12807
- Miguel D, Peckruhn M, Elsner P. Treatment of cutaneous pseudolymphoma: A systematic review. Acta Derm Venereol. 2018;98(3):310–317. doi: 10.2340/00015555-2841
- Bailey NG, Elenitoba-Johnson KS. Molecular diagnostics of T-cell lymphoproliferative disorders. Cancer J. 2014;20(1):48–60. doi: 10.1097/PPO.0000000000000016
- Hristov AC, Comfere NI, Vidal CI, Sundram U. Kappa and lambda immunohistochemistry and in situ hybridization in the evaluation of atypical cutaneous lymphoid infiltrates. J Cutan Pathol. 2020;47(11):1103–1110. doi: 10.1111/cup.13858
- Sanchis-Sánchez C, Santos-Alarcón S, Benavente-Villegas FC, et al. Red nodule on the face with “spontaneous” regression. An Bras Dermatol. 2017;92(5 Suppl 1):135–137. doi: 10.1590/abd1806-4841.20175540
- Han B, Liu H, Wang H. A case of multiple nodular cutaneous B-cell pseudolymphoma successfully treated with glucocorticoid, methotrexate, and hydroxychloroquine. Dermatol Ther. 2022:35(11):e15812. doi: 10.1111/dth.15812
- Allison RR, Moghissi K. Photodynamic Therapy (PDT): PDT Mechanisms. Clin Endosc. 2013;46(1):24–29. doi: 10.5946/ce.2013.46.1.24
- Besch-Stokes JG, Patel MH, Brumfiel CM, et al. Cutaneous B cell pseudolymphoma treated with rituximab and methotrexate. Dermatol Online J. 2021;27(9). doi: 10.5070/D327955138
- Balode D, Beļajeva L, Ruesseler V, et al. Diagnostic challenges and treatment options for cutaneous T cell pseudolymphoma: A case study with rituximab treatment. Am J Case Rep. 2020;(21):e919616. doi: 10.12659/AJCR.919616
- Baumgartner-Nielsen J, Lorentzen H. Imiquimod 5%: A successful treatment for pseudolymphoma. Acta Derm Venereol. 2014;94(4):469. doi: 10.2340/00015555-1730
Supplementary files

